CASE20250528_001
Distal Tip Inflation Technique Gone Too Far: A Risky Maneuver for Severely Calcified Annulus
By Soo Yeon An
Presenter
Soo Yeon An
Authors
Soo Yeon An1
Affiliation
Asan Medical Center, Korea (Republic of)1,
View Study Report
CASE20250528_001
TAVR - Complex TAVR
Distal Tip Inflation Technique Gone Too Far: A Risky Maneuver for Severely Calcified Annulus
Soo Yeon An1
Asan Medical Center, Korea (Republic of)1,
Clinical Information
Relevant Clinical History and Physical Exam
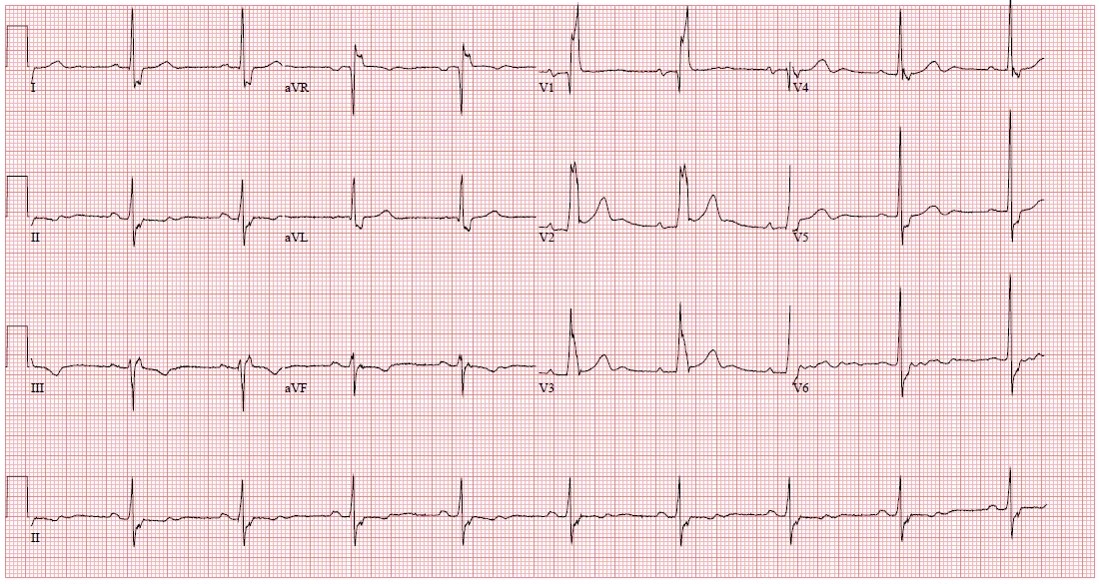
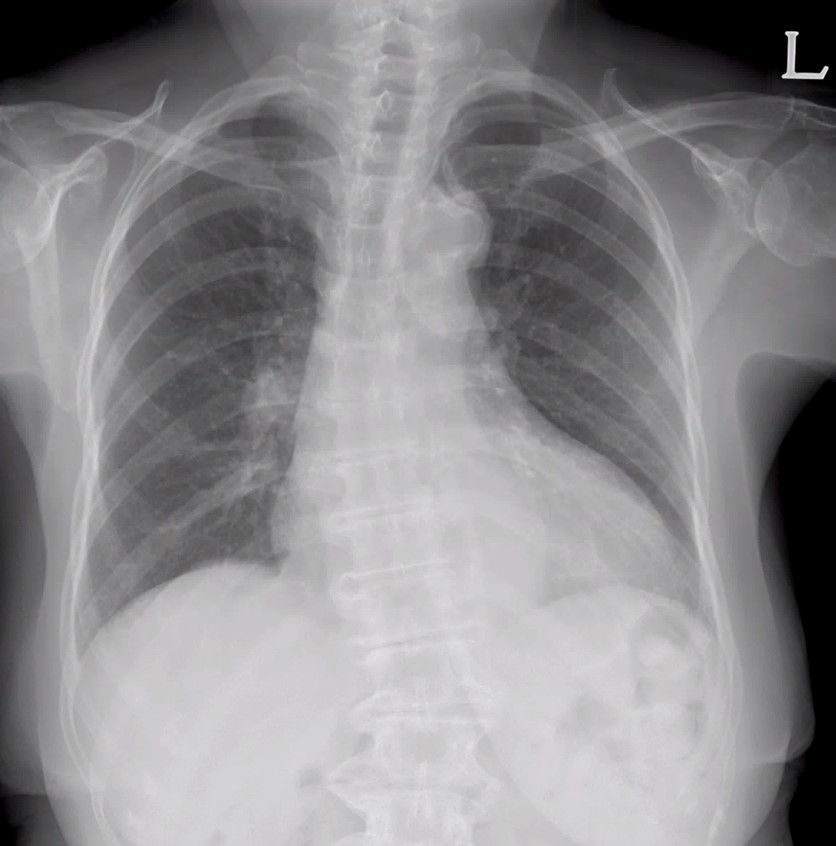
An 83-year-old female with a medical history significant for diabetes mellitus was admitted due to progressively worsening dyspnea on exertion, classified as NYHA Functional Class II. Clinical evaluations including electrocardiography, chest radiography, and routine laboratory testing were conducted upon admission. The Society of Thoracic Surgeons (STS) score was calculated at 6.12%, indicating elevated surgical risk.

Relevant Test Results Prior to Catheterization
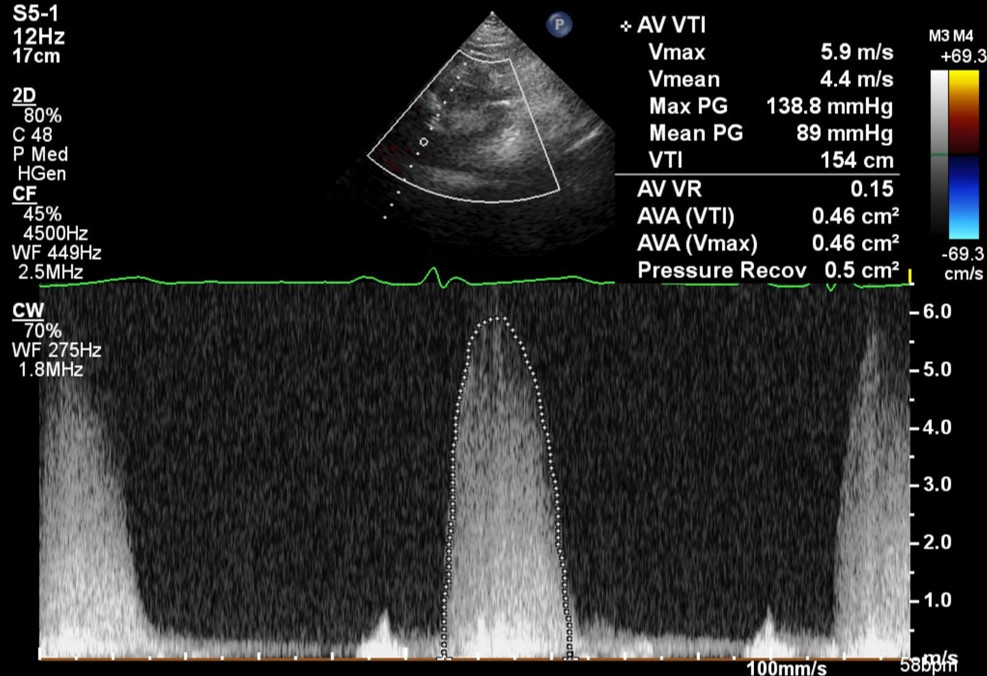
Echocardiography revealed severe aortic stenosis characterized by an aortic valve area of 0.44 cm², with a peak gradient of 143 mmHg and a mean gradient of 90 mmHg. Transaortic valve velocity (Vmax) was notably elevated at 6.0 m/s, and the annulus measured 20 mm in diameter. Left ventricular ejection fraction was preserved at 68%, with concomitant mild aortic regurgitation.
 3_1_TTE_PLAX.mp4
3_1_TTE_PLAX.mp4
3_2_TTE_PSAX.mp4
Relevant Catheterization Findings
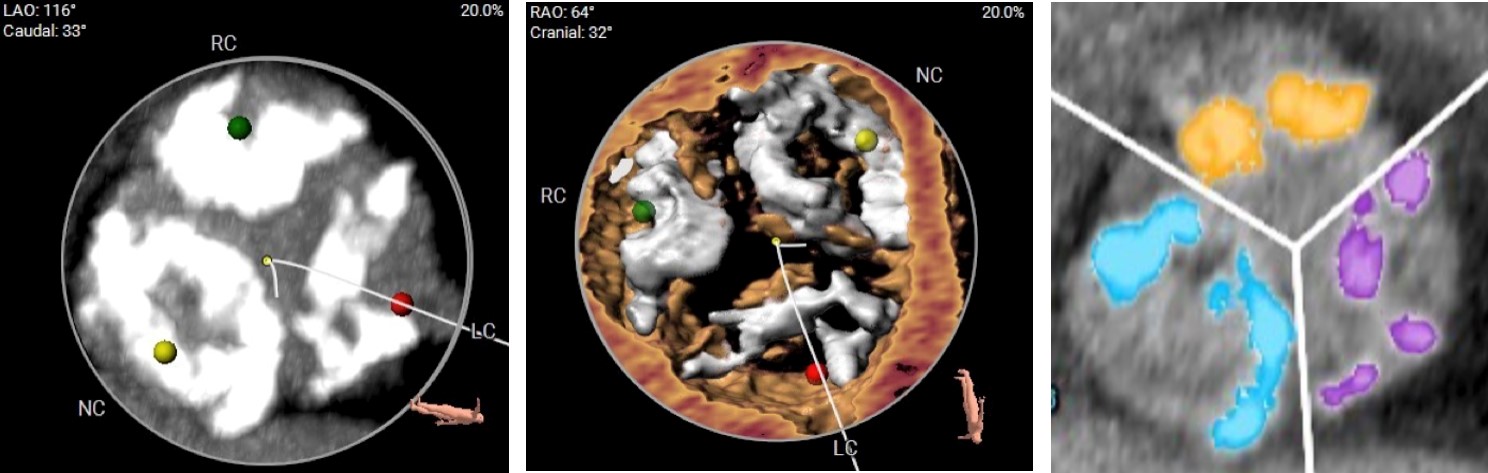
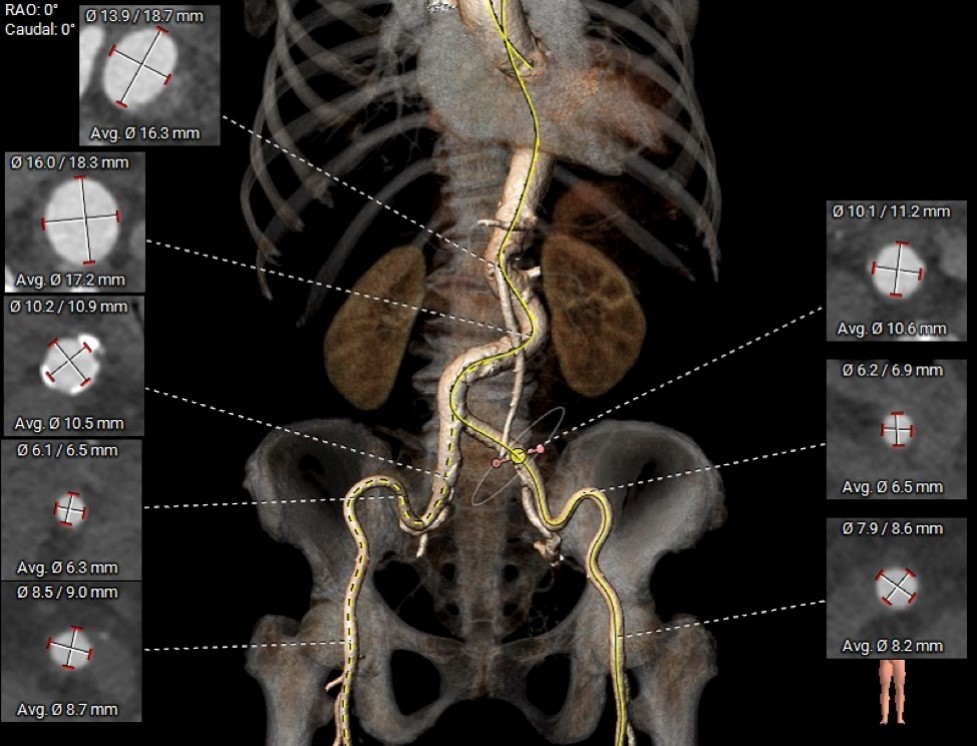
The annulus area measured 423.0 mm², with a perimeter of 74.9 mm and an area-derived annulus diameter of 23.2 mm. Computed tomography demonstrated significant annular calcification. The calcium burden was quantified at 1317 mm³. Coronary artery heights were measured as follows: left coronary artery at 13.0 mm and right coronary artery at 15.2 mm. A mean sinus-to-annulus area ratio of 1.87 and a mean sinotubular junction-to-annulus area ratio of 1.52. The minimal diameters of the external iliac arteries were adequate for femoral access (left 6.2 mm, right 6.1 mm), but both iliac arteries exhibited significant tortuosity.
Interventional Management
Procedural Step
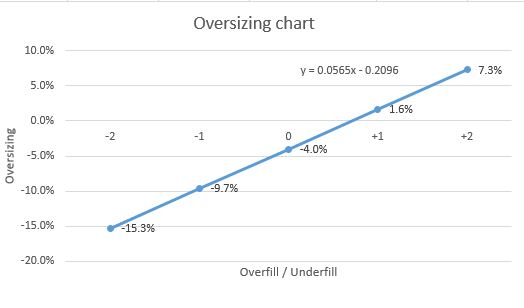
TAVR was performed via femoral arterial access using a 23-mm Edwards SAPIEN 3 valve with a +2cc balloon overfill and -4% undersizing due to heavy annular calcification. Initially, the valve encountered significant resistance during crossing despite pre-dilation with an 18-mm Z-MED balloon. Multiple attempts employing push-and-pull techniques were unsuccessful. Upon consultation with a panel expert, the distal tip inflation technique was employed. Contrary to standard practice, the balloon was inflated to a greater degree (approximately 5 cc), effectively expanding the severely calcified annulus and allowing the valve to cross. This high-risk maneuver resulted in partial displacement of the balloon, necessitating re-centering and re-inflation. Ultimately, valve positioning was successfully achieved with minimal paravalvular leakage. The final angiography showed minor leakage, yet pressure gradients indicated proper valve function, suggesting leakage related primarily to calcification.TAVR is increasingly performed in patients unsuitable for open surgical replacement. Techniques addressing heavily calcified, difficult-to-cross valves have been well studied and documented. Mastery and flexible application of these techniques tailored to individual patient anatomies can significantly enhance TAVR success rates and improve clinical outcomes.
5_1_preballoon.avi
5_2_tip inflate.avi
5_3_post.avi
Case Summary
This case illustrates the distal tip inflation technique during TAVR for a severely calcified aortic valve annulus. Although this approach carries significant risk of device dislodgement and embolization, careful execution facilitated successful valve deployment during complex TAVR procedures.