CASE20250510_001
Graded Coronary Non Compliant Balloon Atrial Septostomy Technique Rescue Severe Refractory Pulmonary Hypertension in Patient with Antiphospholipid Syndrome and Recurrent Pulmonary Emboli, Along with Chronic Thromboembolic Pulmonary Hypertension Following Pulmonary Endarterectomy
By Wittawat Wattanasiriporn
Presenter
Wittawat Wattanasiriporn
Authors
Wittawat Wattanasiriporn1
Affiliation
Rajavithi Hospital, College of Medicine, Rangsit University, Bangkok Thailand, Thailand1,
View Study Report
CASE20250510_001
Other Interventions - Other Interventions
Graded Coronary Non Compliant Balloon Atrial Septostomy Technique Rescue Severe Refractory Pulmonary Hypertension in Patient with Antiphospholipid Syndrome and Recurrent Pulmonary Emboli, Along with Chronic Thromboembolic Pulmonary Hypertension Following Pulmonary Endarterectomy
Wittawat Wattanasiriporn1
Rajavithi Hospital, College of Medicine, Rangsit University, Bangkok Thailand, Thailand1,
Clinical Information
Relevant Clinical History and Physical Exam
38-year-old Thai male
BP 165/119 mmHg, HR 98 bpm, RR 24 bpm, T 36.8°C, O2 sat 92% Cardiac: Normal S1, Lound P2, no murmurs
BP 165/119 mmHg, HR 98 bpm, RR 24 bpm, T 36.8°C, O2 sat 92% Cardiac: Normal S1, Lound P2, no murmurs
Relevant Test Results Prior to Catheterization
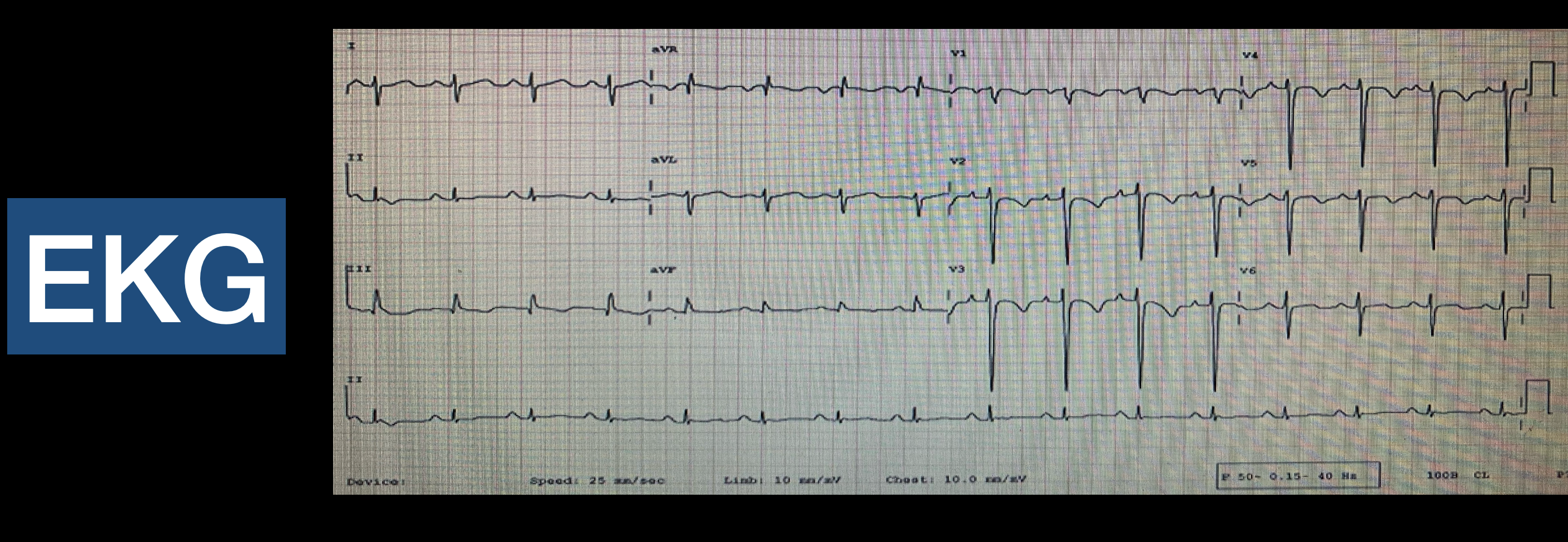
EKG: NSR at 96 bpm, normal axis + 60 degree, no LV hypertrophy, inverted T at V1-V4, non specific st-t change, no arrhythmias CT pulmonary artery: Filling defect with eccentric lesions in anterior and posterior basal segment of right interlobar artery, enlarge pulmonary trunk suspected Pulmonary arterial hypertension.

Relevant Catheterization Findings
CAG: Rt dominant, LCA & RCA normal

Interventional Management
Procedural Step
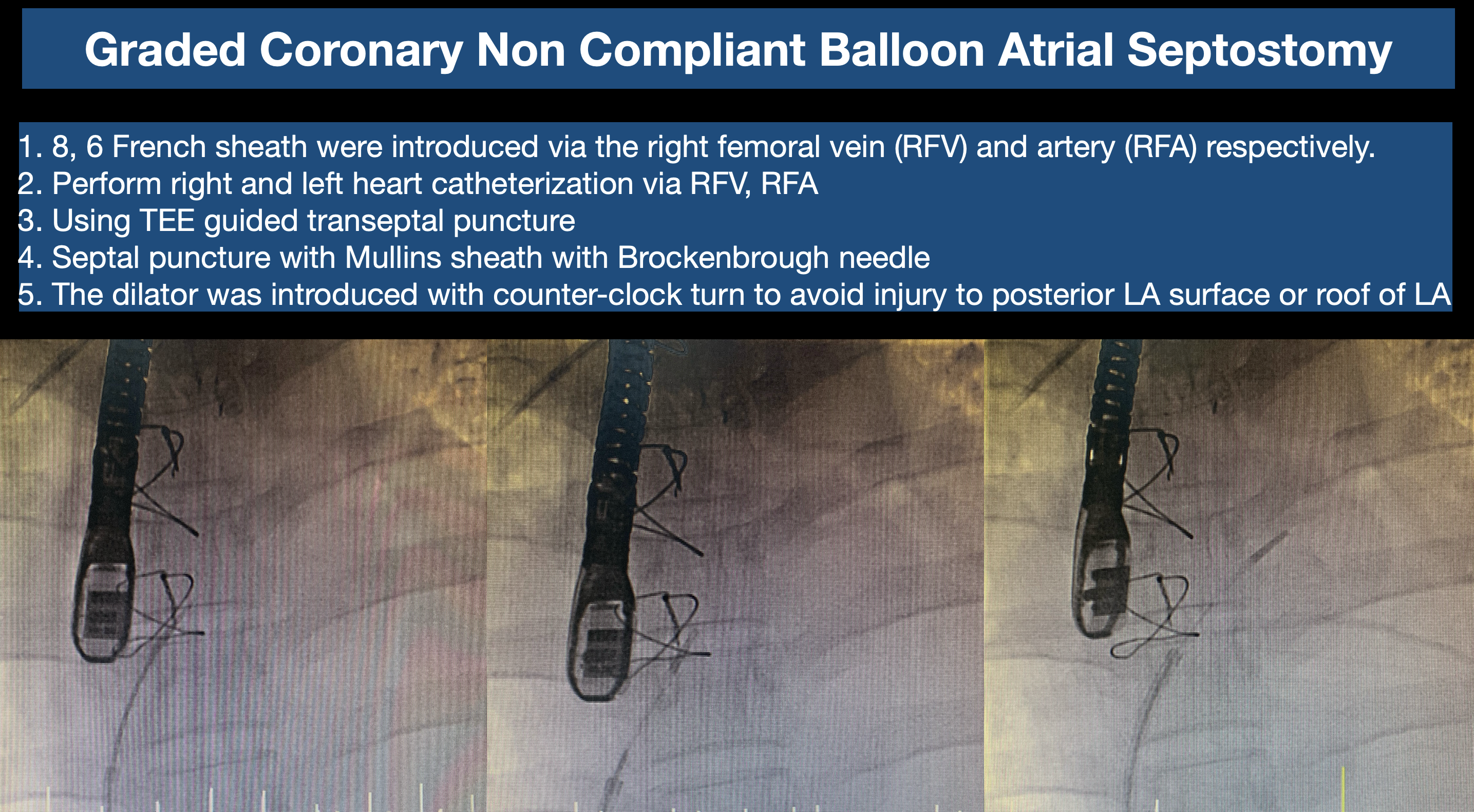
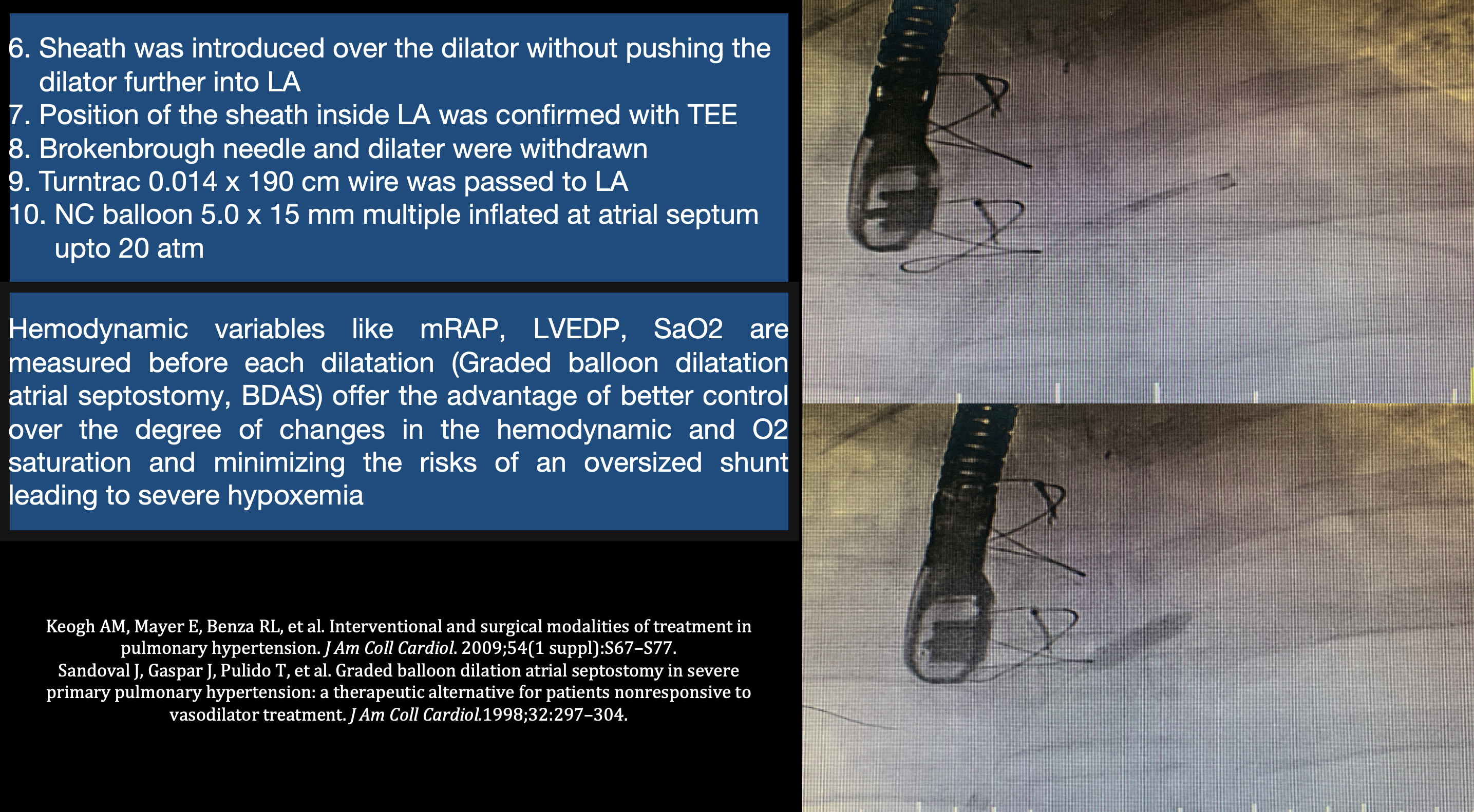
Indication for AS: Severe pulmonary hypertension that is refractory to pulmonary endarterectomy and medication Procedural details 1. 8, 6 French sheath were introduced via the right femoral vein (RFV) and artery (RFA) respectively.