CASE20250509_002
The First Leadless Pacemaker in a Patient with Unrepaired Complex Dextro-Transposition of the Great Arteries
By Tse-Wei Chen
Presenter
Tse-Wei Chen
Authors
Tse-Wei Chen1
Affiliation
National Cheng Kung University Hospital, Taiwan1,
View Study Report
CASE20250509_002
Other Interventions - Other Interventions
The First Leadless Pacemaker in a Patient with Unrepaired Complex Dextro-Transposition of the Great Arteries
Tse-Wei Chen1
National Cheng Kung University Hospital, Taiwan1,
Clinical Information
Relevant Clinical History and Physical Exam
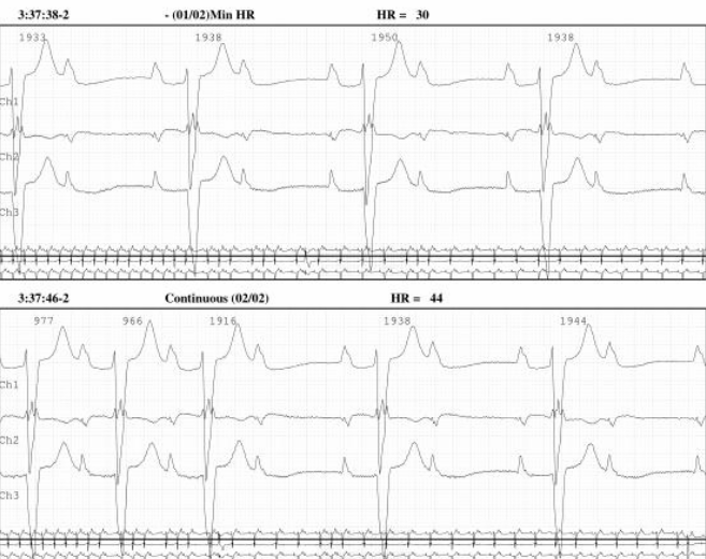
A 37-year-old woman with unrepaired dextro-transposition of the great arteries (d-TGA), end-stage renal disease, diabetes mellitus, and hypertension. She presented with symptomatic high-degree AV block. Her anatomy includes a large VSD (3.5 cm), small secundum ASD, severe pulmonary stenosis, and left atrial dysfunction. Prior PPM was removed due to pocket infection. Recently received Micra AV in the functional RV for mechanical atrial sensing and ventricular pacing.

Relevant Test Results Prior to Catheterization
The patient had a Permcath (tunneled dialysis catheter) in the right subclavian vein, limiting traditional pacemaker options. Prior CT and chest X-ray confirmed that leads would enter the anatomical left ventricle, which serves as the physiological right ventricle in this patient with unrepaired d-TGA and a large VSD, complicating standard pacing strategies.
 Micra-TGA_20240618_V.2.mp4
Micra-TGA_20240618_V.2.mp4
Relevant Catheterization Findings
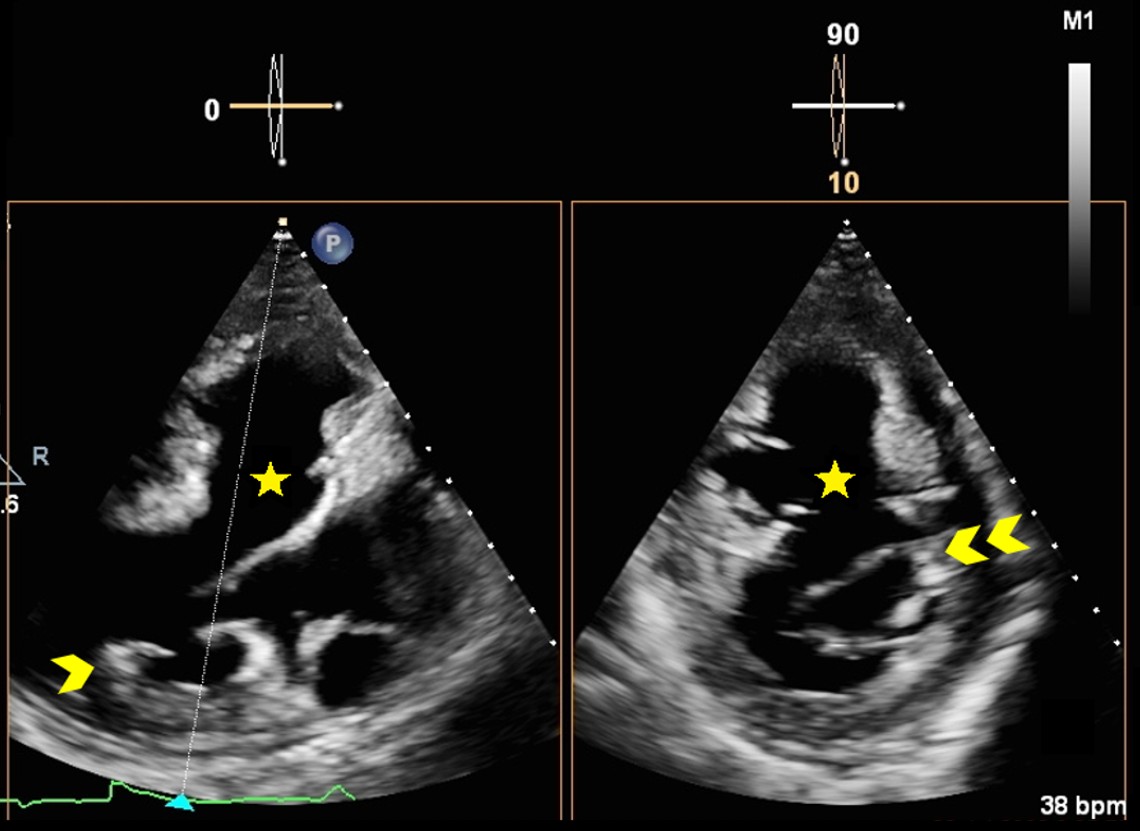
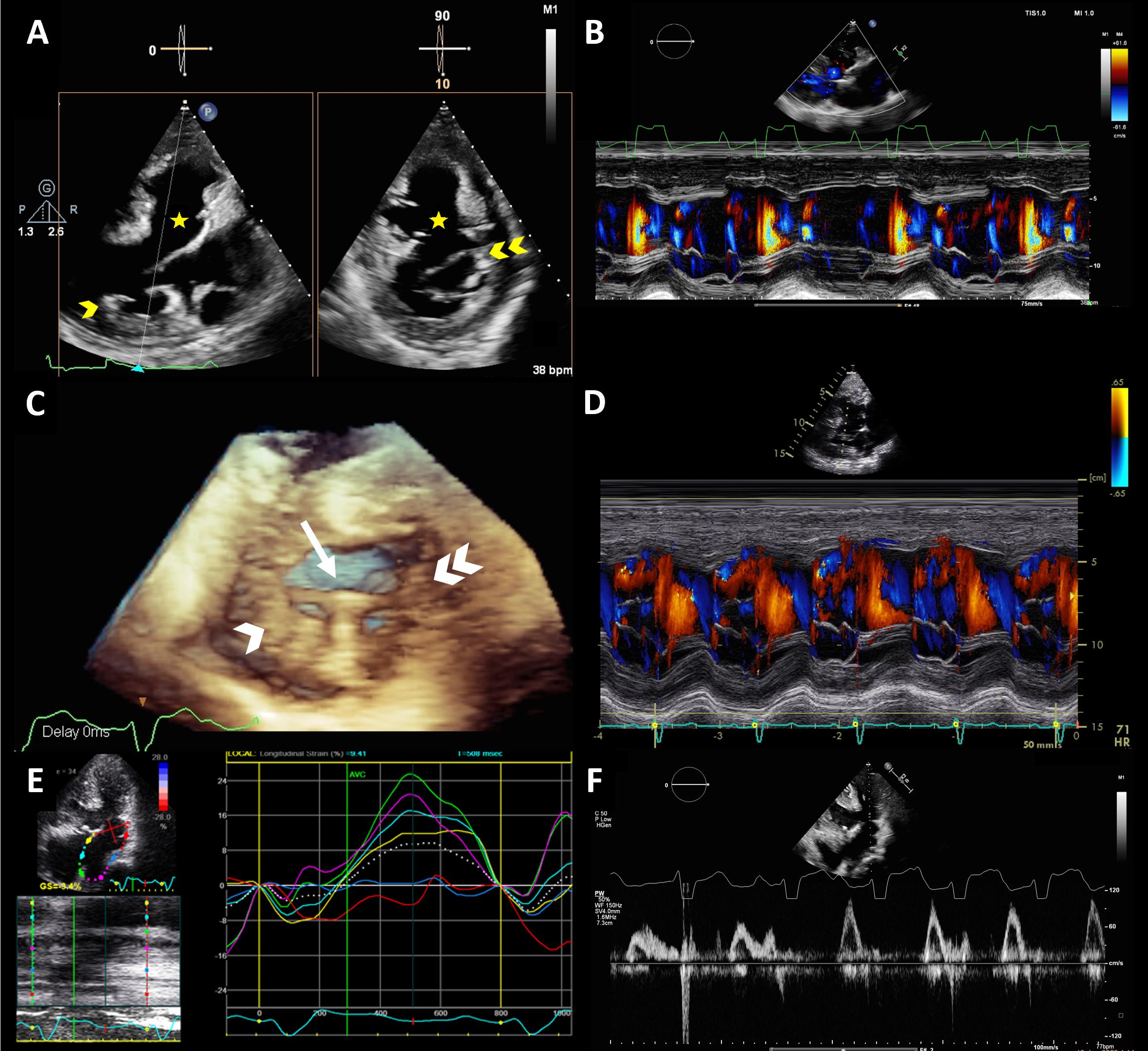
The Micra catheter was navigated through the right atrium and smoothly advanced into the anatomical left ventricle via the large VSD. Initial positioning attempts resulted in tip displacement, but with echocardiographic guidance, the device was successfully anchored between the papillary muscles, ensuring stable deployment within the functional right ventricle.
61393508(8).mp4
JACC video.mp4
Interventional Management
Procedural Step
The patient underwent leadless pacemaker (Micra AV) implantation for complete AV block with limited access due to a right-sided Permcath and a prior pocket infection on the left. Under local anesthesia with 2% xylocaine, right femoral vein access was obtained. A 14 Fr introducer sheath was advanced into the right atrium, and a 23 Fr Micra delivery system was positioned into the anatomical left ventricle (functional right ventricle) via a large VSD.
Initial attempts at device deployment resulted in the Micra tip dislodging, but successful re-deployment was achieved between the papillary muscles with echocardiographic guidance. Passive fixation was confirmed, with excellent capture threshold (0.4 V), impedance (530 Ω), and sensing (3.9 mV). The device was tested under multiple biplane views with satisfactory electrical performance.The introducer was then removed, and hemostasis was achieved without complications. The patient tolerated the procedure well, with no immediate adverse events noted. The Micra AV was confirmed to be functioning appropriately in the VDD mode, supporting effective mechanical atrial sensing and ventricular pacing.
Untitled video - Made with Clipchamp.mp4
Initial attempts at device deployment resulted in the Micra tip dislodging, but successful re-deployment was achieved between the papillary muscles with echocardiographic guidance. Passive fixation was confirmed, with excellent capture threshold (0.4 V), impedance (530 Ω), and sensing (3.9 mV). The device was tested under multiple biplane views with satisfactory electrical performance.The introducer was then removed, and hemostasis was achieved without complications. The patient tolerated the procedure well, with no immediate adverse events noted. The Micra AV was confirmed to be functioning appropriately in the VDD mode, supporting effective mechanical atrial sensing and ventricular pacing.
Case Summary
This case highlights the successful implantation of a Micra AV leadless pacemaker in a patient with complex congenital heart disease, including unrepaired dextro-transposition of the great arteries (d-TGA) with a large VSD. The leadless approach was essential due to prior pocket infection and a right-sided Permcath, limiting conventional pacemaker options. The Micra AV was securely deployed within the functional right ventricle, achieving stable electrical parameters and effective atrioventricular synchrony.