CASE20250504_001
Noncoronary Sinus Pivot Implantation Technique for Transcatheter Aortic Valve Replacement with Venus A-Plus Valve in a Patient with Pure Native Aortic Regurgitation
By Yi Xu, Xianwu Lan, Zicheng Li
Presenter
Yi Xu
Authors
Yi Xu1, Xianwu Lan1, Zicheng Li1
Affiliation
First Affiliated Hospital of Ji'Nan University, China1,
View Study Report
CASE20250504_001
TAVR - Complex TAVR
Noncoronary Sinus Pivot Implantation Technique for Transcatheter Aortic Valve Replacement with Venus A-Plus Valve in a Patient with Pure Native Aortic Regurgitation
Yi Xu1, Xianwu Lan1, Zicheng Li1
First Affiliated Hospital of Ji'Nan University, China1,
Clinical Information
Relevant Clinical History and Physical Exam
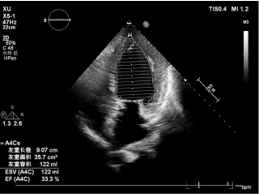
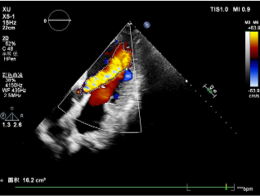
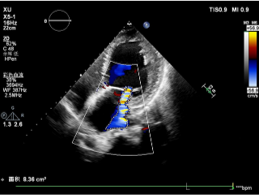
A 70-year-old female was admitted to our hospital due torecurrent chest tightness and shortness of breath for 2 years, worsened for 1week. His comorbidities include hypertension, hyperlipidemia, andhyperuricemia. PE found Grade 4 diastolic murmur in the right 2nd ICS. ECGshowed complete left bundle branch block. Echocardiogram showed severeaortic regurgitation (VC 8.5mm, EROA 0.49cm2, volume 85ml) with mildto severe mitral regurgitation. LVEF was significantly reduced (33%).
Relevant Test Results Prior to Catheterization
Pre-operative CT angiography showed tricuspid aortic valve with pureregurgitation. There was no calcification. The mean aortic annulus diameter was23.5mm and the perimeter was 74.6mm, with an area of 427.5 mm2. Thesinus of Valsalva diameter was 30.9, 28.5, and 31.0 mm for the left, right, andnoncoronary cusps, respectively. Coronary heights were 9.4mm (left) and 13.9mm(right). The STJ diameter was 31.4mm. Ascending aorta maximum diameter was 40.5mm.The heart angle was 73°.
 11.mp4
11.mp4
Relevant Catheterization Findings
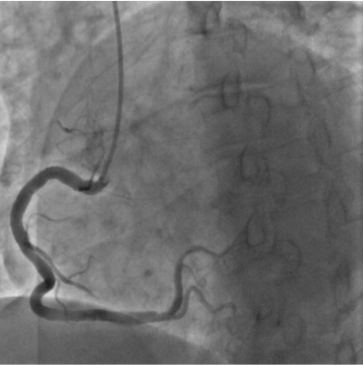
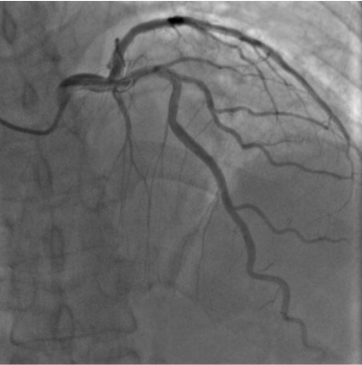
Coronary angiography showed no significant stenosis in left and right coronary arteries.
Interventional Management
Procedural Step
The procedure was conducted under generalanathesia. Left femoral artery puncture was obtained and a6-Fr sheath wasplaced. Right femoral artery was punctured under angio-guidance andanother 6-Fr sheath was placed. The right 6-Fr sheath was then replaced by a10-Fr one. Temporary pacing wire was placed through left femoral vein. Theaortic valve was crossed with wire under guidance of an AL2 catheter. A PIGcatheter was exchanged and basal pressures were measured. The 10-Fr sheath wasreplaced by a 20-Fr sheath. A L29 Venus-A-Plus self-expandable valve (VenusMedtech, Hangzhou, China) was loaded and transmitted to the aortic root. The firstattempt to deploy at zero position failed as the valve slipped towards the ventricle.We tried a second time using noncoronary sinus pivot implantation (NCPI)technique succeeded and the valve was released 2mm above the bottom ofnoncoronary sinus. A slightly downward force was exerted by the physician toavoid slippery and misplacement of the valve. Transesophageal echocardiogramwas also performed to ensure the location of the valve before it was fullydeployed. Aortic root angiogram was repeated, showing good placement andexpansion of the valve. Post-procedural echocardiogram showed no sign of aorticregurgitation and only mild mitral regurgitation. The ejection fraction wasalso improved to 36%. The patient recovered well and was discharged 5 daysafter the procedure.
1.avi
2.avi
10.mp4
Case Summary
This case demonstrates successful TAVR using the NCPI technique with Venus A-Plus self-expandable valve in a patient with pure aortic regurgitation (PAR). This supports the NCPI technique as a valuable alternative for traditional method in certain PAR patients.