CASE20240716_006
Where There’s a Will, There’s a Way
By Hansu Park
Presenter
Hansu Park
Authors
Hansu Park1
Affiliation
Asan Medical Center, Korea (Republic of)1,
View Study Report
CASE20240716_006
TAVR - Complex TAVR
Where There’s a Will, There’s a Way
Hansu Park1
Asan Medical Center, Korea (Republic of)1,
Clinical Information
Relevant Clinical History and Physical Exam
A 75-year-old male presented with recurrent syncope and dyspnea on exertion. He underwent coronary artery bypass grafting and ascending aorta replacement 9 years ago.

Relevant Test Results Prior to Catheterization
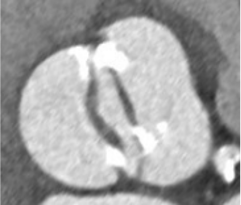
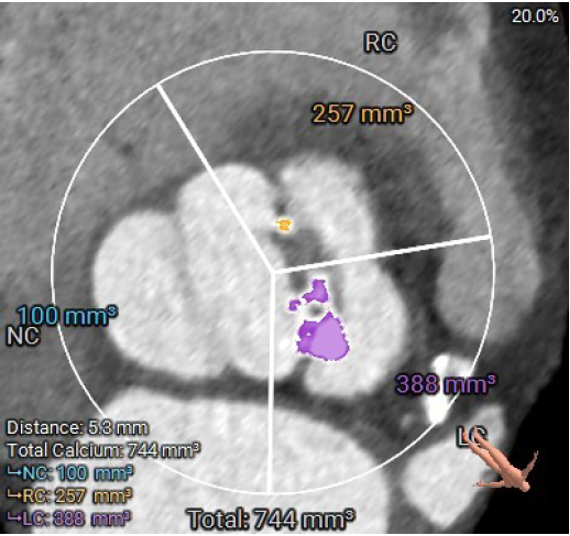
Echocardiography showed a bicuspid valve with severe aortic stenosis and mildly reduced LV function (EF 48%). The STS score was 4.5%. the area of the annulus was measured in 575mm² with a type I bicuspid valve. The calcium score and coronary heights to the RCA was 20.7mm and to LCA was 7.9mm. Vascular access to both femoral arteries was sufficient, but the ascending aorta was banded at about 80 degrees, and a horizontal aorta was observed.
Relevant Catheterization Findings
Interventional Management
Procedural Step
During the TAVR procedure, we failed to cross the stenotic aortic valve despite using various wires, as the orifice area was too small. We decided on retrograde wiring via septal puncture. The septal puncture was performed under fluoroscopy guidance, and we attempted retrograde wiring with a Terumo wire (0.035 inches, 260 cm) and a 6Fr wedge balloon catheter. We successfully crossed the aortic valve with the retrograde wire using floating balloon. After retrograde wiring, we tried anterograde wiring using the buddy wire technique but failed. We placed the retrograde wire in the descending aorta. We used a EN snare wire via the femoral sheath to capture the retrograde wire and externalize it. An AL1 catheter was introduced over the retrograde wire and into the left ventricle. We then used an Safari wire and advanced it into the LV cavity via the AL1 catheter.Pre-ballooning was done with a 20-mm Z-med balloon, and a 26-mm Sapien S3 ultra valve was positioned. After implantation, acute AR occurred followed by cardiac arrest. CPR was performed for one cycle, and we attempted post-ballooning with the valve balloon. After post-ballooning, the patient recovered. The final aortogram showed a well-apposed prosthetic valve with no significant aortic regurgitation.
 Han Su Park - 5-1.mp4
Han Su Park - 5-1.mp4
Han Su Park - 5-2.mp4
Han Su Park - 5-3.mp4
Case Summary
Balloon expandable valve is the better option for horizontal aorta. In difficult AV wiring case, we can consider the retrograde approach. We should do the preparation with pre-ballooning enough in Heavy calcified Aortic valve.