CASE20240716_005
[Invited Case] An Access Site Consideration After Failing Transfemoral Approach
By Euihong Ko
Presenter
Euihong Ko
Authors
Euihong Ko1
Affiliation
Kokura Memorial Hospital, Japan1,
View Study Report
CASE20240716_005
TAVR - Non-femoral TAVR
[Invited Case] An Access Site Consideration After Failing Transfemoral Approach
Euihong Ko1
Kokura Memorial Hospital, Japan1,
Clinical Information
Relevant Clinical History and Physical Exam
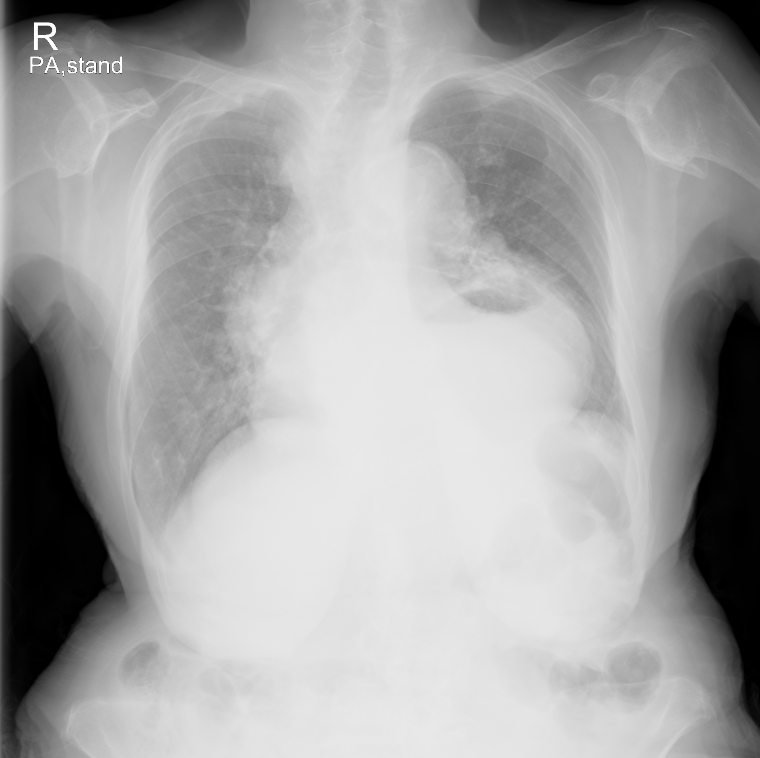
A 94-year-old female with very severe aortic stenosis (AS) presented to our institution with worsening dyspnea over preceding week. Chest X-ray showed cardiomegaly and congestion (Figure 1). Transthoracic echocardiography demonstrated well preserved ejection fraction and very severe AS with peak velocity of 5.91 m/s, and mean PG of 85.2 mmHg. The Society of Thoracic Surgery score was 5.065%. Clinical frailty scale was 4. She had a history of hypertension, hyperlipidemia, and hypothyroidism.
Relevant Test Results Prior to Catheterization
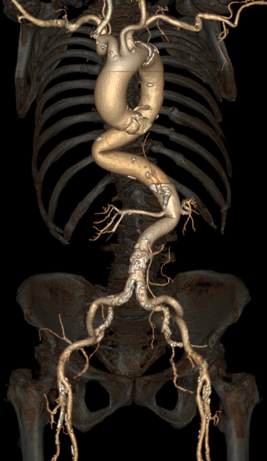
Computed tomography showed an annulus area of 368mm2, a perimeter of 69.9 mm, and small aortic root with Sinus of Valsalva (LCC: 237.3mm, RCC: 26.5mm, NCC: 28.9mm). The aortic valve was tricuspid and demonstrated severe calcification in RCC and NCC. The bilateral iliac arteries were more than 6 mm in diameter, however there was tortuous angular portion at thoracoabdominal aorta (Figure 2).
Relevant Catheterization Findings
Interventional Management
Procedural Step
A 23 mm Evolut FX was selected due to severe calcification. The patient received local anesthesia in combination with intravenous opioids. A 4Fr pigtail was inserted via left femoral artery. Then, we tried to advance an 18Fr GORE DrySeal Flex Introducer Sheath 65 cm via right femoral artery but couldn’t cross the tortuous angular portion. We exchanged wire from Amplatz Extra-Stiff to Lunderquist Extra-stiff wire, however this didn’t work. Therefore, we inserted another Lunderquist Extra-stiff wire through the pigtail of contralateral side, and finally succeeded in crossing the tortuous portion and advanced Gore DrySeal to the descending aorta (Video 1). We preformed predilation with the aortic Inoue-Balloon catheter (Toray, Tokyo, Japan) of 20 mm. Then we tried to deliver Evolut FX but it was stuck in the GORE DrySeal (Video 2). Given the better crossability, we tried with NAVITOR 23mm but in vain. Our heart team decided to perform transcarotid TAVR owing to the presence of almost no plaque in the left common carotid artery (CCA), and brain magnetic resonance angiography revealed good communications between the anterior and posterior communicating arteries. Transcarotid TAVR was successfully done using SAPIEN 3 Ultra RESILIA 23 mm (-2cc) with the 30-min clamp time of the left CCA (Video 3).
 Video 1 DrySeal delivery.mp4
Video 1 DrySeal delivery.mp4
Video 2 Evolut failure.mp4
Video 3 S3UR.mp4
Case Summary
Transcarotid access is a safe and feasible approach in a case requiring an alternative approach. Furthermore, brain MRA and INVOS could be useful to evaluate the communications of cerebral arteries and monitor cerebral local circulation during CCA clamping for the purpose of preventing cerebral vascular accidents.