CASE20240708_001
Breaking Barriers: Transcarotid TAVR in Practice
By Faisal Yousef Almajid
Presenter
Faisal Yousef Almajid
Authors
Faisal Yousef Almajid1
Affiliation
Asan Medical Center, Kuwait1,
View Study Report
CASE20240708_001
TAVR - Non-femoral TAVR
Breaking Barriers: Transcarotid TAVR in Practice
Faisal Yousef Almajid1
Asan Medical Center, Kuwait1,
Clinical Information
Relevant Clinical History and Physical Exam
• 77M, BMI 26.3 / BSA 1.76 • Chief complaints- DOE (NYHA Fc II)• Medical history. Severe degenerative AS, preserved LV function. LM Bifurcation PCI. Rt Vertebral artery stenosis (severe)• STS score = 2.49%, Euroscore II = 1.22%

Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
Interventional Management
Procedural Step
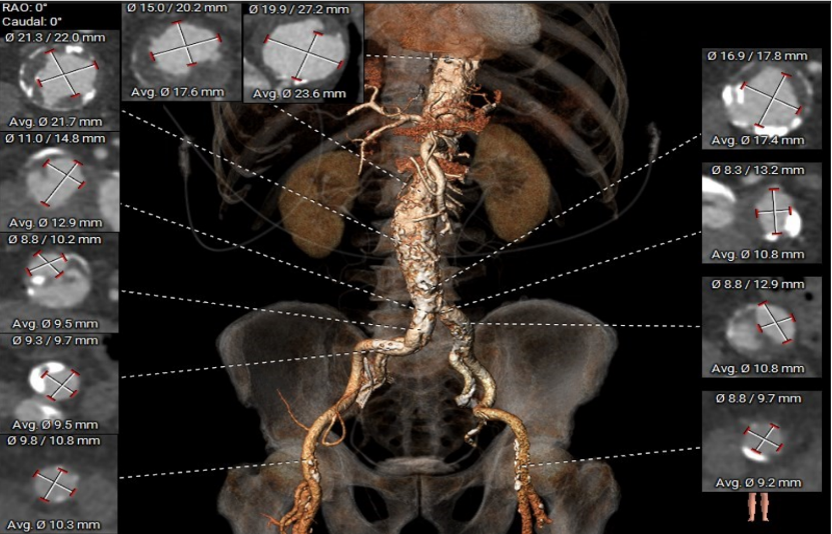
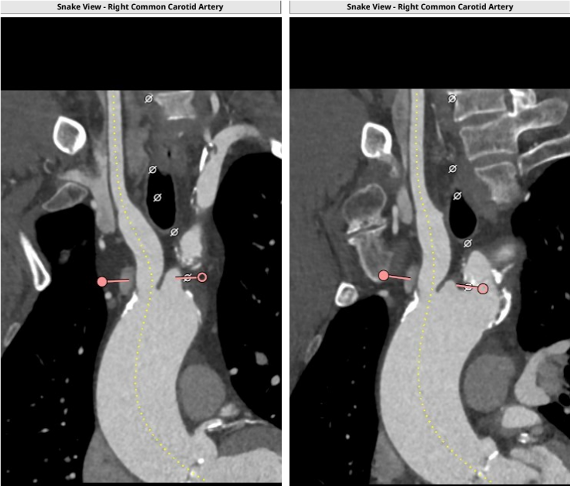
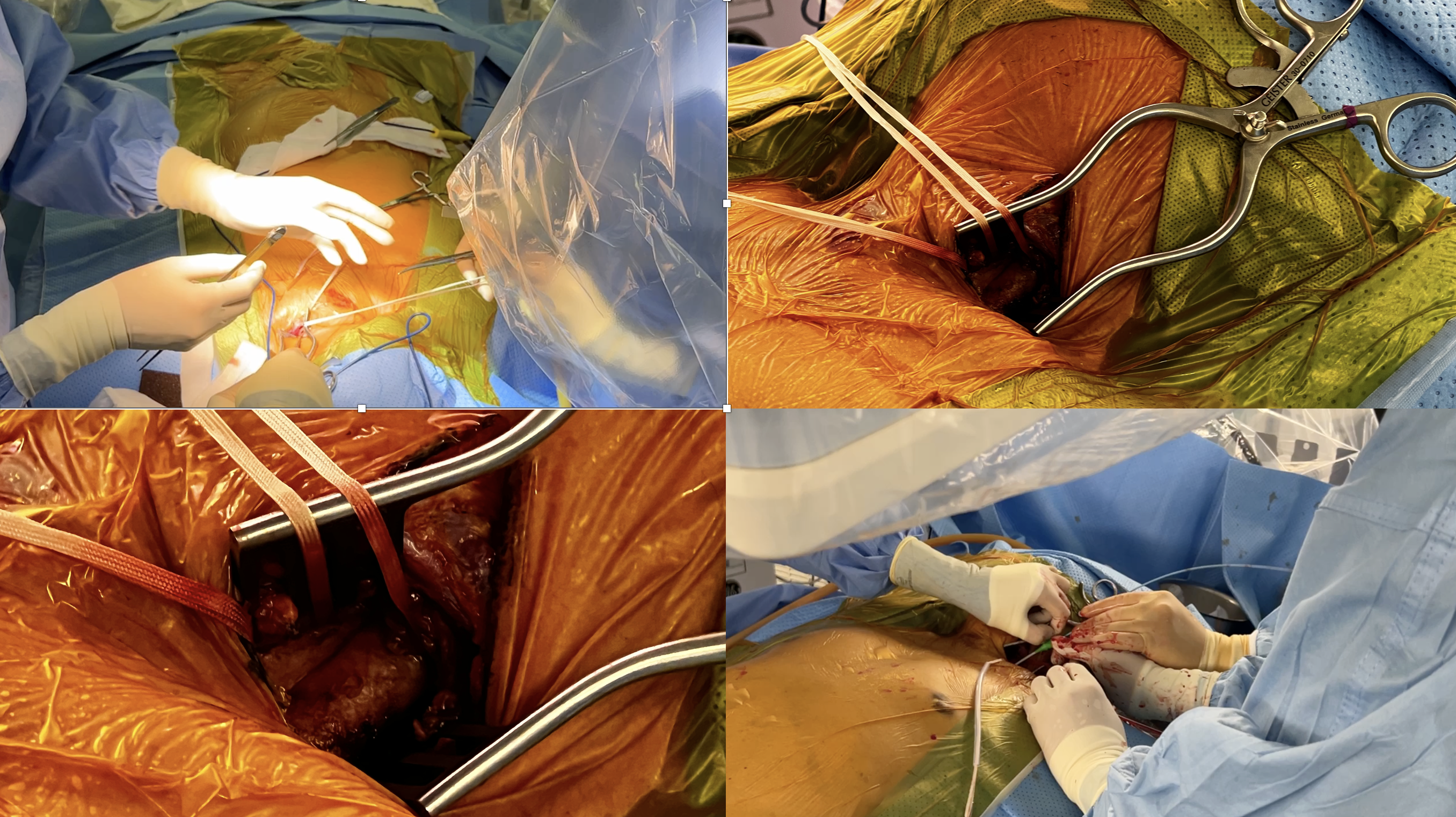
Annulus area was 609 mm², within the size range of a 29 mm Sapien S3 valve. Area ratios for SOV, LVOT, and STJ were within acceptable limits.Calcium score is 1,466 requiring predilation. Coronary heights were acceptable. Femoral artery Segmentation showed bilateral iliofemoral dissection, requiring an alternate route. Left subclavian analysis showed a tortuous vessel with a minimal diameter of 5.0 mm, making it not feasible. Left common carotid analysis showed a tortuous vessel with a minimum diameter of 5.8 mm. The right common carotid was chosen for having a minimum diameter of 6.1 mm and a more straightforward trajectory.MRI showed severe stenosis of the right vertebral artery and a hypoplastic A1 segment of the anterior communicating artery, indicating more supply from the left carotid. Therefore, right carotid access was more feasible. We set up our hybrid room with operators on the right side of the patient’s head to facilitate right carotid access.Due to heavy calcification, our target oversizing for a 29 mm S3 valve was 5-10%. We predilated using a 22 mm balloon, then went nominal with a 6.6% area oversize. Our cardiac surgeon performed the cutdown. Avoiding vagal nerve injury, the proximal carotid was identified, punctured, and the e-sheath inserted. We crossed the valve using a JR catheter. Valve alignment was performed in the ascending aorta, followed by usual TAVR steps. Predilation with a 22 mm balloon was done, and the valve was deployed.
 Video 1.mp4
Video 1.mp4
Video 2.mp4
Case Summary
• Transcarotid TAVR at AMC is feasible with proper CT analysis, room preparation, and a multidisciplinary team.• This technique reduces vascular complications and improves efficiency, but delivery system choice is crucial.• Trans-Carotid access is a promising second-line option for our TAVR population and is expected to enhance outcomes as expertise grows.