CASE20240524_001
Fixing Double Trouble in an Octogenarian with Acute Heart Failure
By Sakolwat Montrivade, Akara Kijnithikul, Wasant Soonfuang, Sukhum Tachasakunjaroen, Anuruck Jeamanukoolkit
Presenter
Sakolwat Montrivade
Authors
Sakolwat Montrivade1, Akara Kijnithikul1, Wasant Soonfuang1, Sukhum Tachasakunjaroen1, Anuruck Jeamanukoolkit1
Affiliation
Police General Hospital, Thailand1,
View Study Report
CASE20240524_001
Mitral Valve Intervention - TEER
Fixing Double Trouble in an Octogenarian with Acute Heart Failure
Sakolwat Montrivade1, Akara Kijnithikul1, Wasant Soonfuang1, Sukhum Tachasakunjaroen1, Anuruck Jeamanukoolkit1
Police General Hospital, Thailand1,
Clinical Information
Relevant Clinical History and Physical Exam
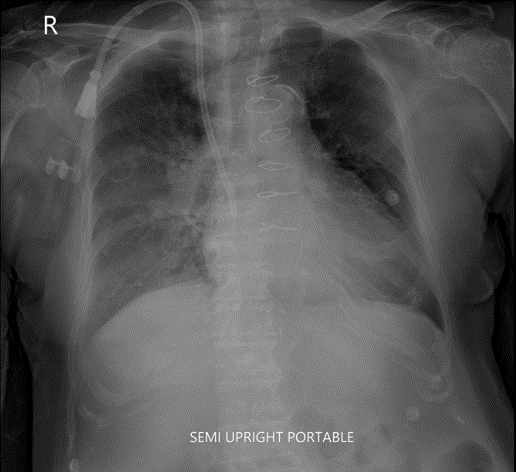
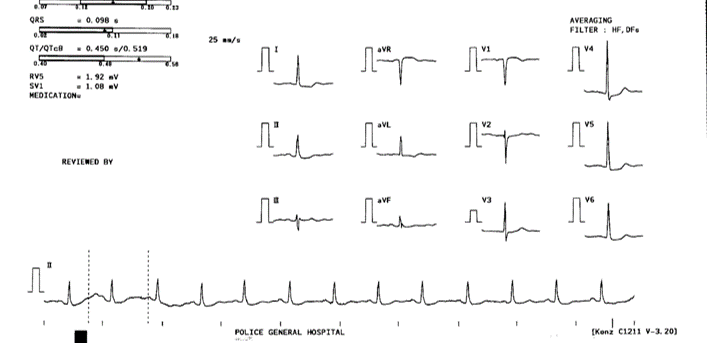
An 80-year-old woman with PMH of CAD post CABG, T2DM, HTN, CKD on dialysis presented with acute heart failure. She was immediately intubated upon arrival. Her vitals were stabilized with BP of 160/80 mmHg, HR of 90/min and SpO2 of 92%. Cardiac examination revealed elevated JVP, normal S1S2 and PSM grade III/VI at apex together with bilateral rales. Hs-troponin T was 1,000 ng/mL and TTE showed LVEF of 50%, hypokinesis in inferior wall and severe MR. The diagnosis of NSTEMI with HF was made.
Relevant Test Results Prior to Catheterization
TEE showed mitral valve prolapse in A2-P2 segments and flail posterior mitral valve leaflet causing severe anteriorly directed jet MR. The anatomy of MR was suitable for TEER. We brought the patient to the catheterization lab and performed CAG which revealed occluded LAD and LCX, severe stenosis in mid RCA with heavy calcification and severe stenosis in PDA. LIMA to LAD was patent but SVG to OM was occluded and SVG to PDA had severe stenosis at distal anastomosis.
 1.2.840.113663.1500.1.522821014.3.21.20231221.131950.199.dcm.wmv
1.2.840.113663.1500.1.522821014.3.21.20231221.131950.199.dcm.wmv
1.2.840.113663.1500.1.522821014.3.27.20231221.132252.199.dcm.wmv
WEB_1.3.12.2.1107.5.4.5.121528.30000023121300051360200000395.4.512.dcm.wmv
Relevant Catheterization Findings
We opted to PCI of RCA and PDA. Rotational atherectomy was done at proximal to mid RCA using Rota Burr 1.5 mm, 180,000 rpm for 5 runs. We then further predilated the lesion with NC balloon 3.0 mm at 18-22 atm. Distal RCA was stented with EES 3.0 x 33 mm. Mid RCA was stented with EES 3.0 x 48 mm and proximal RCA was stented with EES 3.5 x 33 mm. The stents were post-dilated using 3.5 mm and 4.0 mm NC balloon. Lastly, a paclitaxel coated balloon 2.5 x 25 mm was deployed at PDA lesion.
WEB_1.3.12.2.1107.5.4.5.121528.30000023121300051360200000557.4.512.dcm.wmv
WEB_1.3.12.2.1107.5.4.5.121528.30000023121300051360200000779.4.512.dcm.wmv
WEB_1.3.12.2.1107.5.4.5.121528.30000023121300051360200000780.4.512.dcm.wmv
Interventional Management
Procedural Step
We held a heart team meeting and discussed the treatment of MVP with flail posterior mitral leaflet. The patient was deemed suitable for mitral TEER given 1). high patient's risk profile with NSTEMI, HF, CKD on dialysis, and respiratory failure on mechanical ventilation 2). post sternotomy status 3). optimal MR anatomy with A2-P2 segments, good coaptation length and depth, flail gap of less than 10 mm and flail width of less than 15 mm. We planned to use single NTW MitralClip G4 to appose the leaflets given broad gap and moderate leaflet length.
1.2.840.113663.1500.1.467305539.3.150.20240111.150237.526.dcm.wmv
1.2.840.113663.1500.1.467305539.3.152.20240111.150349.576.dcm.wmv
1.2.840.113663.1500.1.522823475.3.8.20240112.101328.763.dcm.wmv
We brought the patient to the lab and put the patient under general anesthesia. Right femoral venous access was obtained under ultrasound guidance and transeptal puncture at superoposterior position was obtained using electrified Conquest Pro 12 in Brockenbrough needle to avoid needle slippage from bulging LA. MitraClip steerable guide and catheter were advanced in the usual fashion. We successfully grasped A2-P2 segment and a single NTW MitraClip G4 was successfully deployed. There was 1+ residual MR and acceptable mean gradient across MV of 2.5 mmHg. We ended the procedure at this point as placing a second clip might not be of benefit. The patient was transfered to CCU for further HF treatment and discharged home in 7 days.
Case Summary
- In patients with very high risk profile, Mitral Transcatheter Edge-to-Edge Repair (TEER) is an excellent alternative to open mitral valve surgery as we demonstrate a case of NSTEMI and HF with complex coronary anatomy together with severe primary MR from flail leaflet undergoing complex high risk PCI and M-TEER.- Anatomical consideration for M-TEER including A2-P2 position, flail gap of less than 10 mm and flail width of less than 15 mm, is very important in procedural planning and successful deployment of the clip.- Risk and benefit of placing a second clip should be strongly considered in a fragile and high risk patient. Reducing MR from 4+ to 1+ may be enough in those cases.