CASE20240519_001
A Case of Post Surgical Aortic Valve Replacement Paravalvular Leakage; Valve-in-Valve Transcatheter Aortic Valve Replacement with Bioprosthetic Valve Fracture
By Osung Kwon, Junghoon Lee, Daeung Ohn
Presenter
Daeung Ohn
Authors
Osung Kwon1, Junghoon Lee2, Daeung Ohn3
Affiliation
Eunpyeong St. Mary's Hospital, Korea (Republic of)1, Catholic university of Korea, Eunpyeong St. Mary's hospital, Korea (Republic of)2, The Catholic University of Korea Eunpyeong St. Mary's Hospital, Korea (Republic of)3,
View Study Report
CASE20240519_001
TAVR - Valve-in-Valve TAVR
A Case of Post Surgical Aortic Valve Replacement Paravalvular Leakage; Valve-in-Valve Transcatheter Aortic Valve Replacement with Bioprosthetic Valve Fracture
Osung Kwon1, Junghoon Lee2, Daeung Ohn3
Eunpyeong St. Mary's Hospital, Korea (Republic of)1, Catholic university of Korea, Eunpyeong St. Mary's hospital, Korea (Republic of)2, The Catholic University of Korea Eunpyeong St. Mary's Hospital, Korea (Republic of)3,
Clinical Information
Relevant Clinical History and Physical Exam
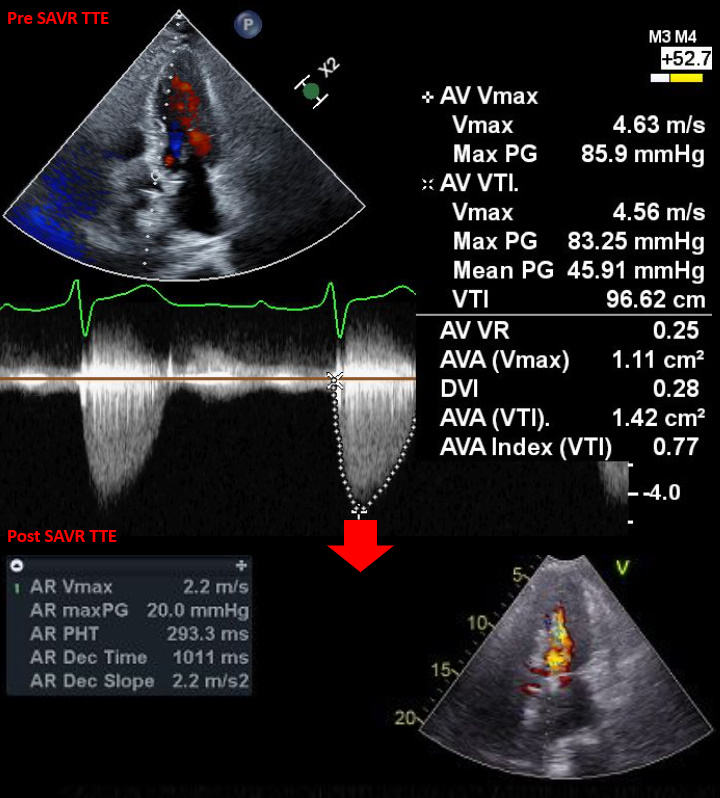
An 80-year-old male patient with a history of diabetes, hypertension, and hyperlipidemia initially presented to the cardiology clinic two years ago with chest pain and dyspnea. He was diagnosed with severe aortic stenosis (AS) and subsequently underwent surgical aortic valve replacement (SAVR). Although he recovered well postoperatively, a paravalvular leak (PVL) remained (Pressure Half Time (PHT) = 293.3 ms).
 1A_preop_TTE.mp4
1A_preop_TTE.mp4
1B_postop_TTE.mp4
Relevant Test Results Prior to Catheterization
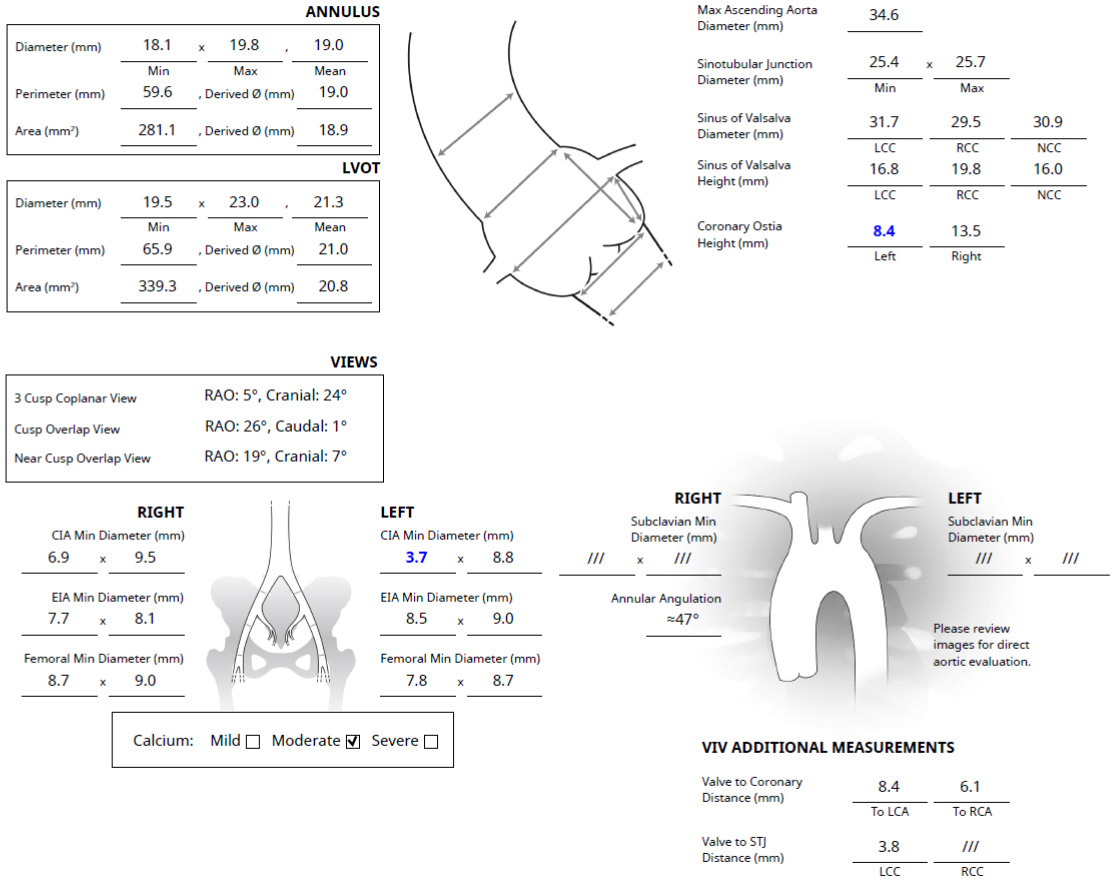
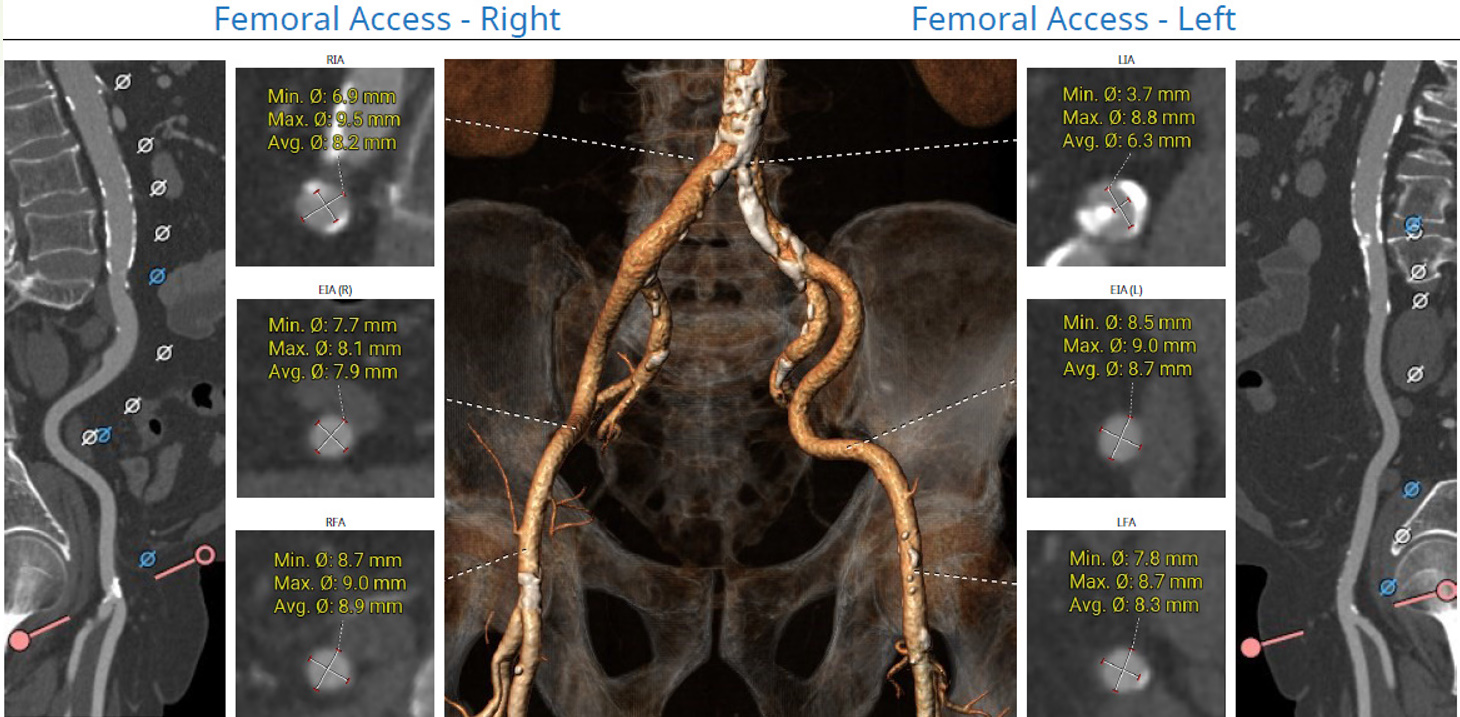
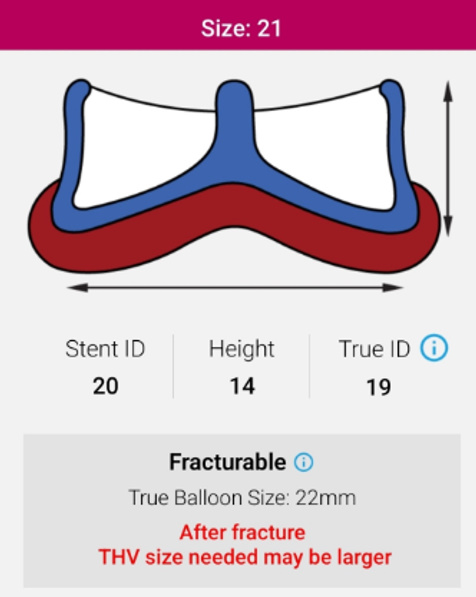
The patient gradually deteriorated over the following year and follow up tests revealed worsening PVL. We recommended performing valve in valve transcatheter aortic valve replacement (TAVR) instead of reoperation. The inner diameter of the 21mm valve used in the patient was 19 mm, so we selected an 23 mm self-expandable valve with 21 % oversizing. The right femoral artery was appropriate as the main approach site, and since the left coronary ostial height was 8.4 mm, we planned for protection.
2A_preTAVR_TEE.mp4
Relevant Catheterization Findings
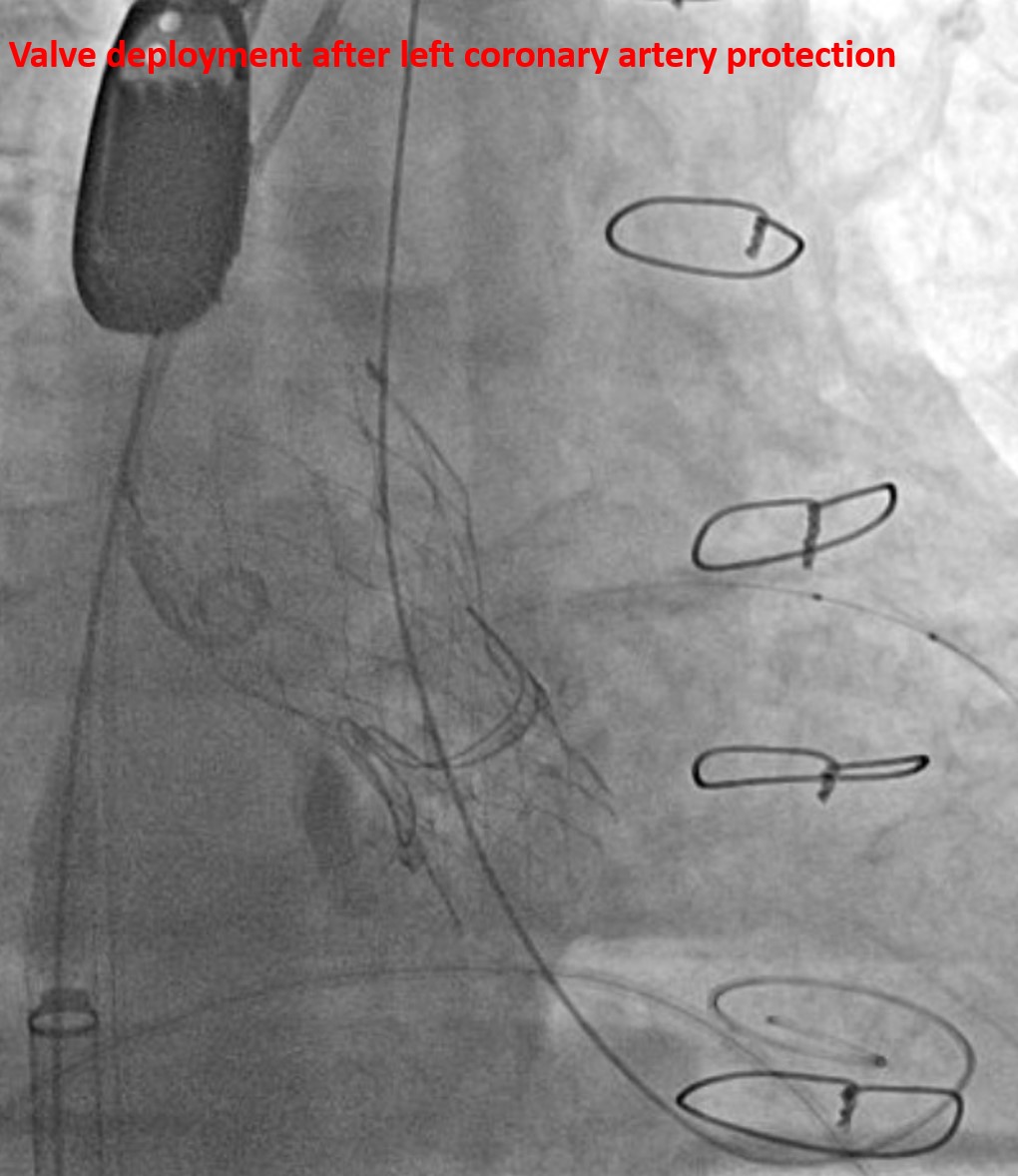
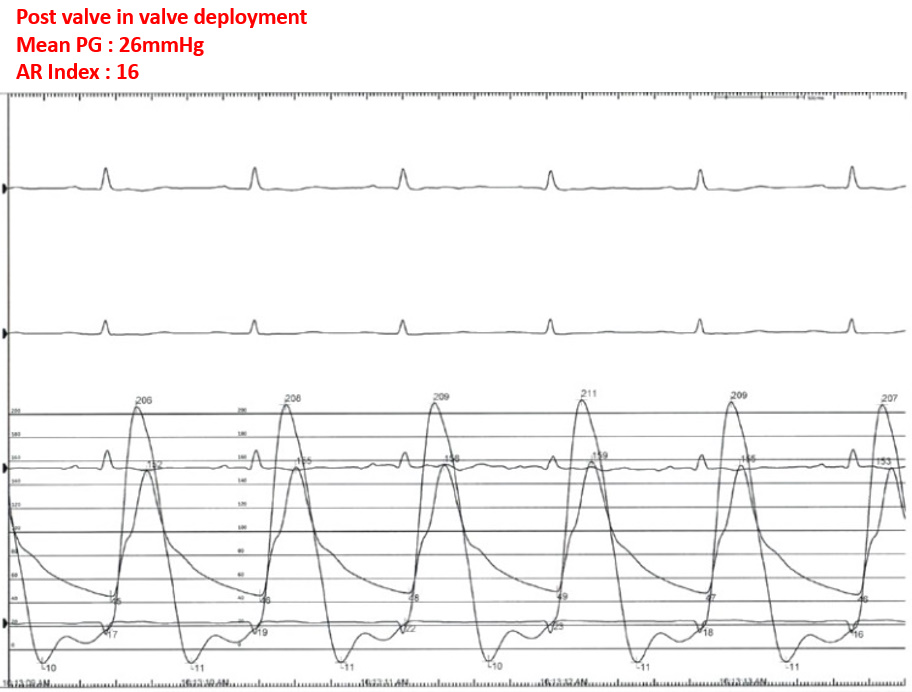
We planned for a target mean pressure gradient (PG) under 20 mmHg with post-TAVR non-compliant (NC) 20 mm ballooning. An NC 22 mm balloon was prepared for potential valve fracture if intra-TAVR transesophageal echocardiography (TEE) showed residual PVL. For left coronary artery protection, a stent was placed before TAVR. TAVR started about 4 mm below the surgical valve stent and was performed smoothly, resulting in an improved mean PG of 26 mmHg and an aortic regurgitation index (ARI) of 16.
Interventional Management
Procedural Step
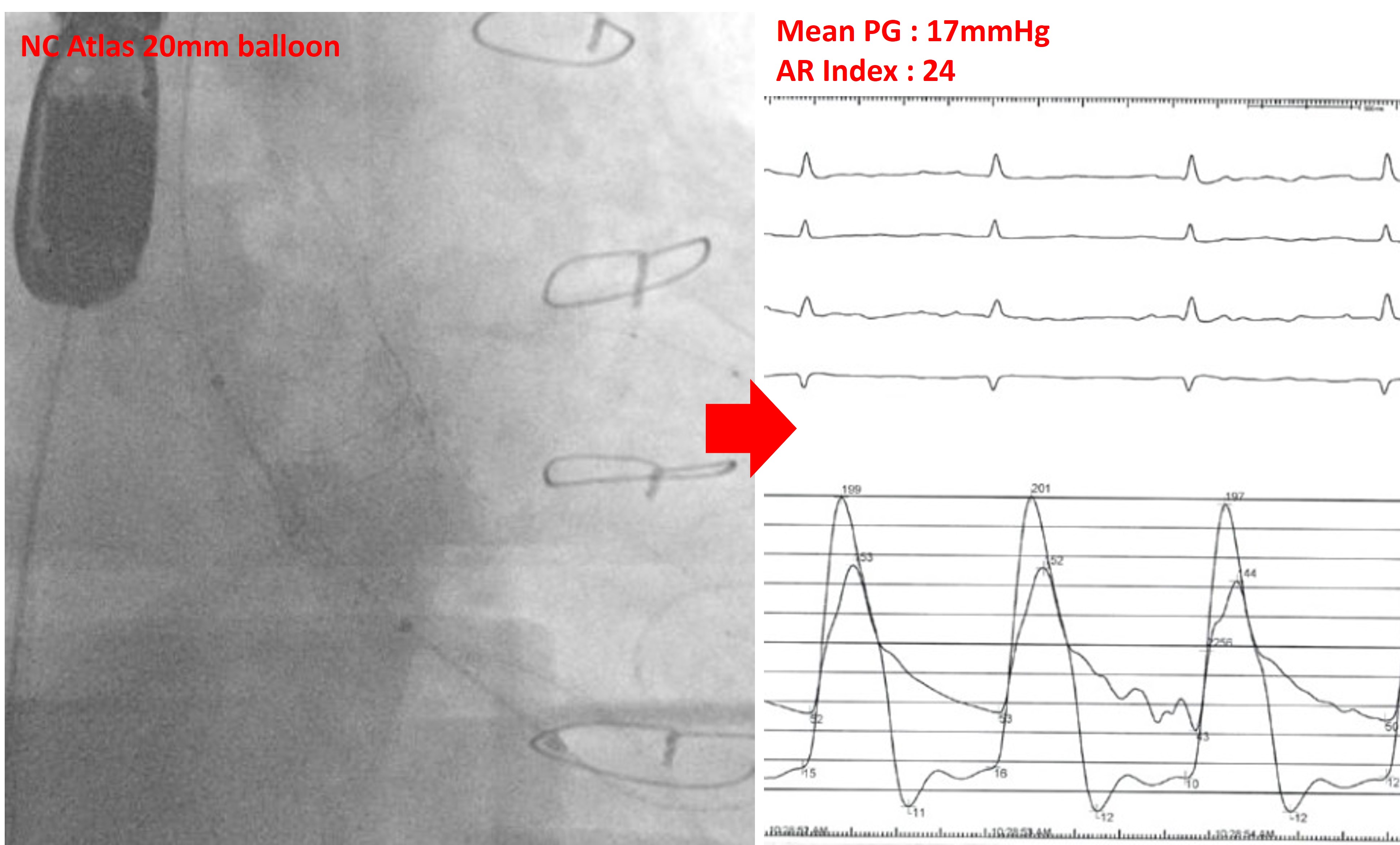
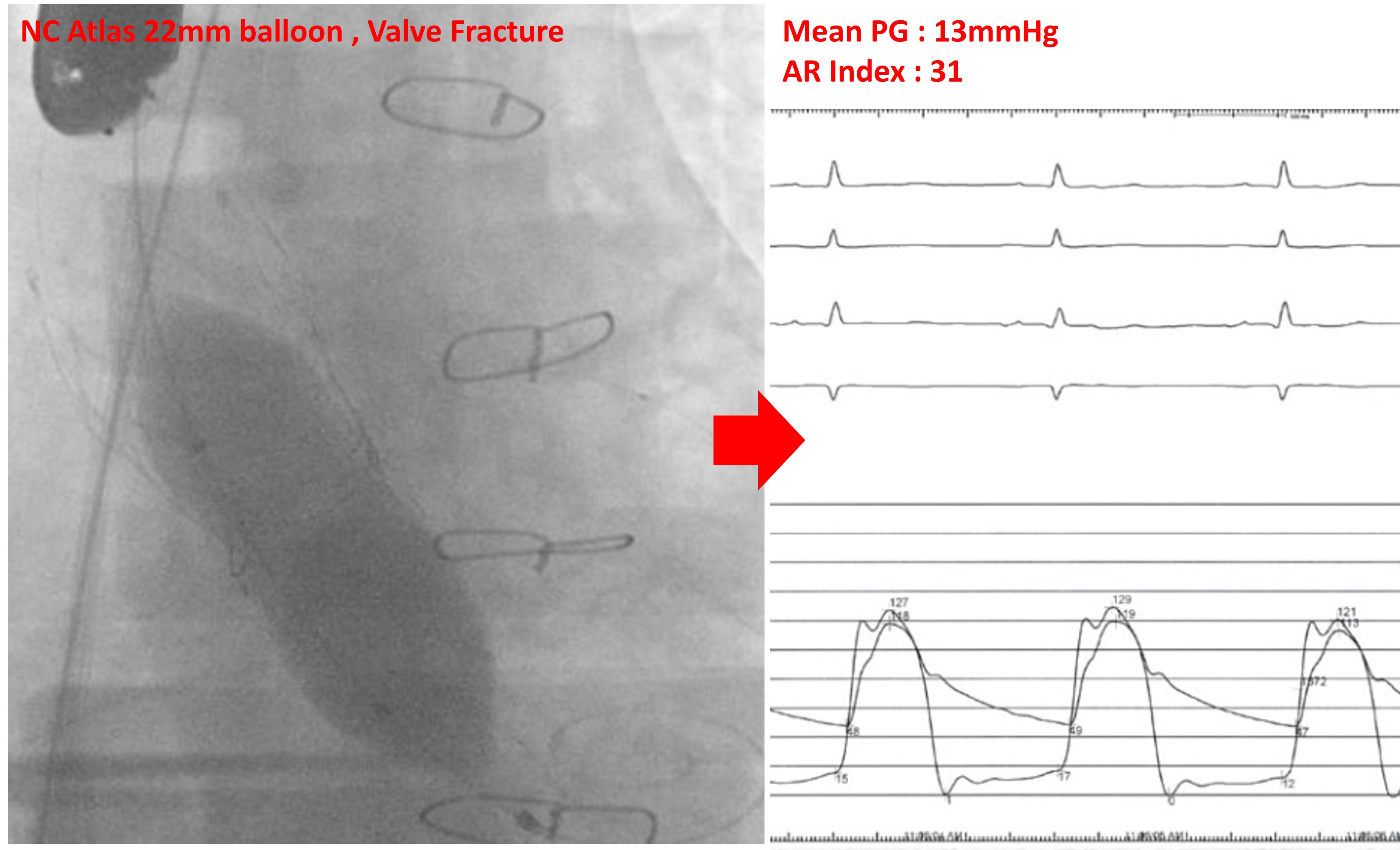
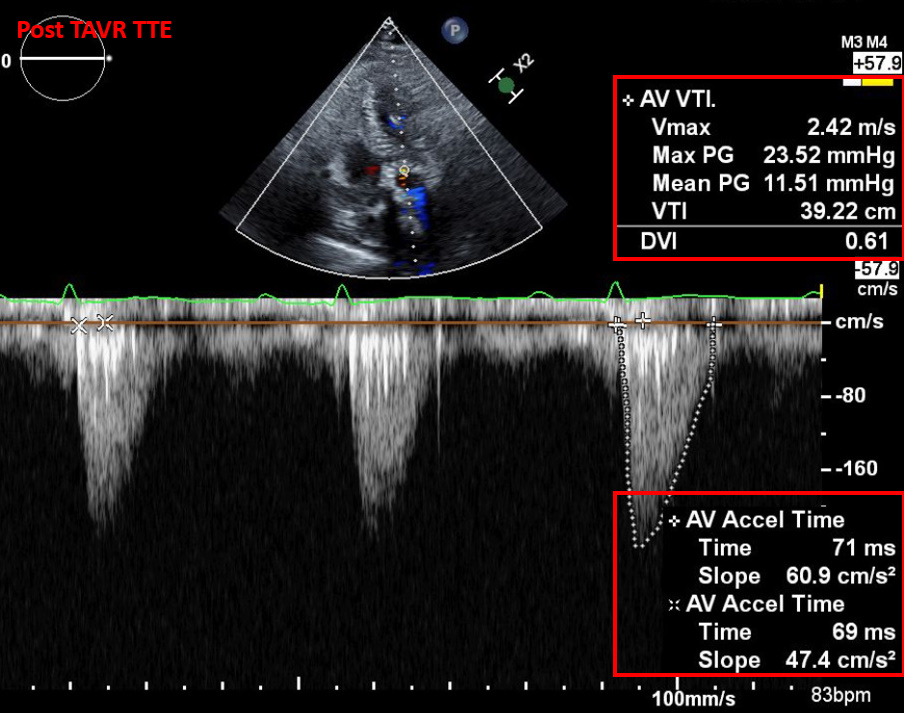
After TAVR deployment, post-TAVR NC 20 mm ballooning was performed with rated burst pressure (16 atmospheres (ATM)), resulting in a mean PG of 17 mmHg and an ARI of 24. Although we considered ending the procedure upon achieving these target values, we decided on additional 22 mm NC ballooning with valve fracture for further correction of PVL. NC 22 mm ballooning with high pressure (18 ATM) was performed, confirming valve fracture via fluoroscopy. This improved the mean PG to 13 mmHg and the ARI to 31. After confirming PVL reduction, we concluded the procedure. Post-TAVR transthoracic echocardiography (TTE) showed no PVL, with favorable results in mean PG and other parameters. The patient was discharged on the second day after the procedure without any notable complications.
Case Summary
We achieved symptomatic and echocardiographic improvement with valve-in-valve TAVR and post-TAVR NC ballooning in a post-SAVR PVL patient. Furthermore, for additional PVL correction, we performed valve fracture and additional ballooning. In cases of the existing surgical valve dysfunction with accompanied PVL, valve in valve TAVR with valve fracture might be a better treatment option. Additionally, further study on the rupture risk estimation or rupture prevention associated with high-pressure ballooning is necessary.