CASE20240429_001
Is There Still a Role for Heterotopic Tricuspid Valve Implantation? - A Case Report in Severe TR Secondary to Post Pacemaker Lead Extraction
By Tsz Ho Chan, Kar Lok Leo Lai, Kent, Chak Yu So, Ka Ho Kevin Kam, Ka Lung Chui, Yat Sun Joseph Chan
Presenter
Tsz Ho Chan
Authors
Tsz Ho Chan1, Kar Lok Leo Lai2, Kent, Chak Yu So2, Ka Ho Kevin Kam2, Ka Lung Chui2, Yat Sun Joseph Chan2
Affiliation
Pok Oi Hospital, Hong Kong, China1, Prince of Wales Hospital, Hong Kong, China2,
View Study Report
CASE20240429_001
Tricuspid Valve Intervention - Tricuspid Valve Intervention
Is There Still a Role for Heterotopic Tricuspid Valve Implantation? - A Case Report in Severe TR Secondary to Post Pacemaker Lead Extraction
Tsz Ho Chan1, Kar Lok Leo Lai2, Kent, Chak Yu So2, Ka Ho Kevin Kam2, Ka Lung Chui2, Yat Sun Joseph Chan2
Pok Oi Hospital, Hong Kong, China1, Prince of Wales Hospital, Hong Kong, China2,
Clinical Information
Relevant Clinical History and Physical Exam
88 years old gentleman, presented with NYHA Class 4 symptoms. His past medical history included hypertension, atrial fibrillation and prostate cancer. He received permanent pacemaker since 30 years ago with interval pacemaker replacement done. Latest replacement complicated with infection which required removal of whole CIED system. Post removal complicated with cardiac tamponade and acute severe TR. Afterwards he was diuretics dependent and suffered from advanced heart failure symptoms
Relevant Test Results Prior to Catheterization
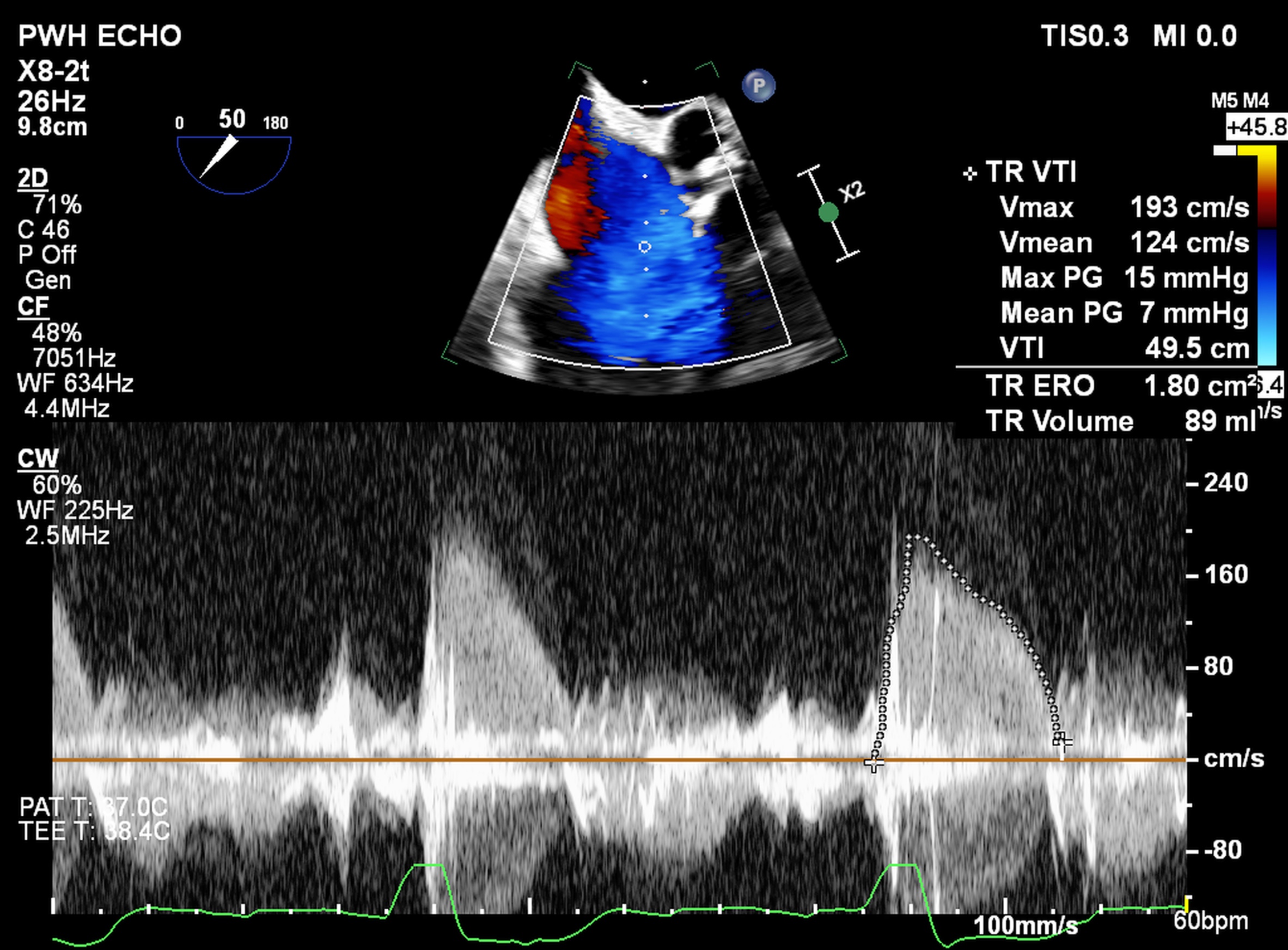
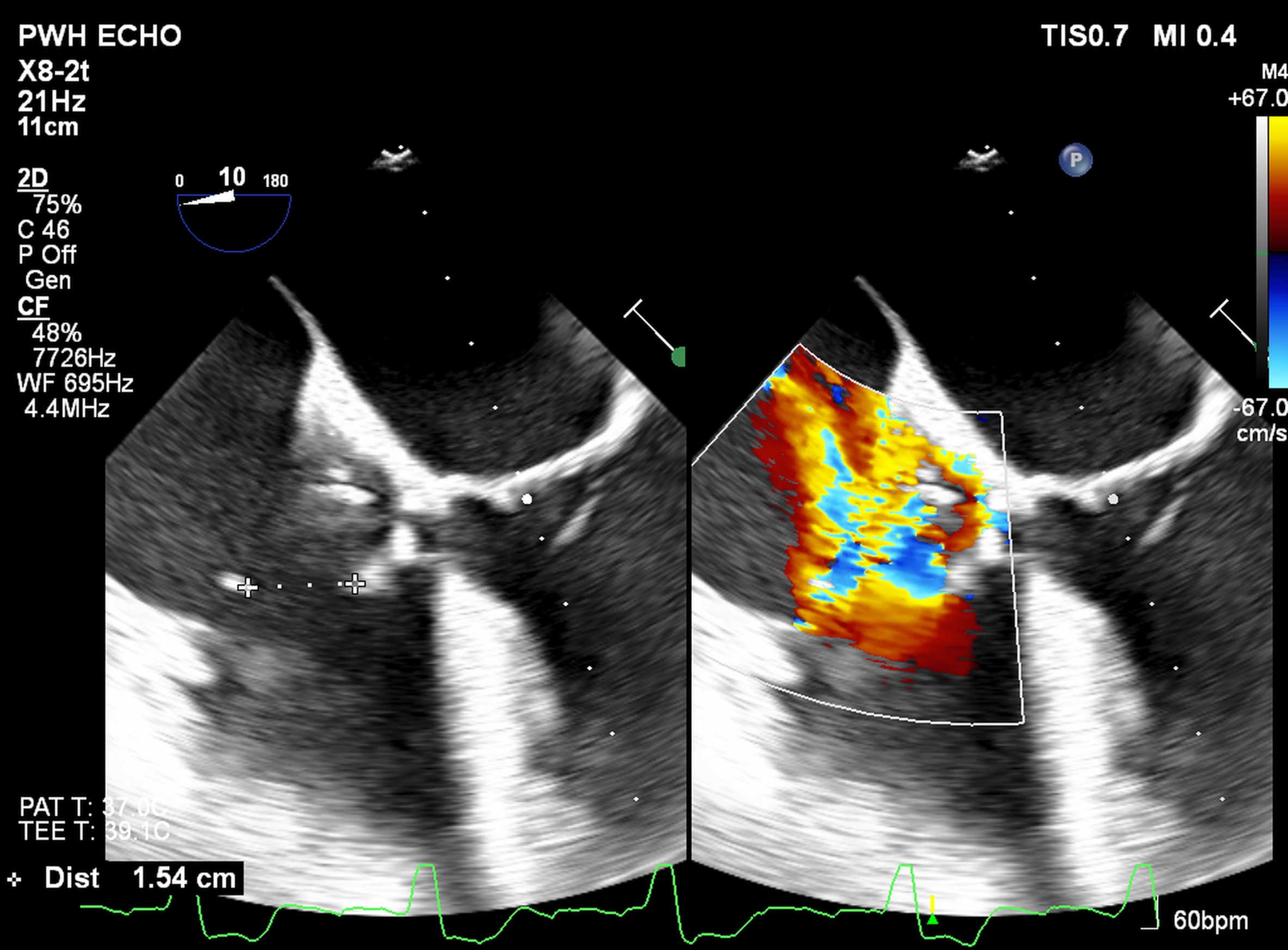
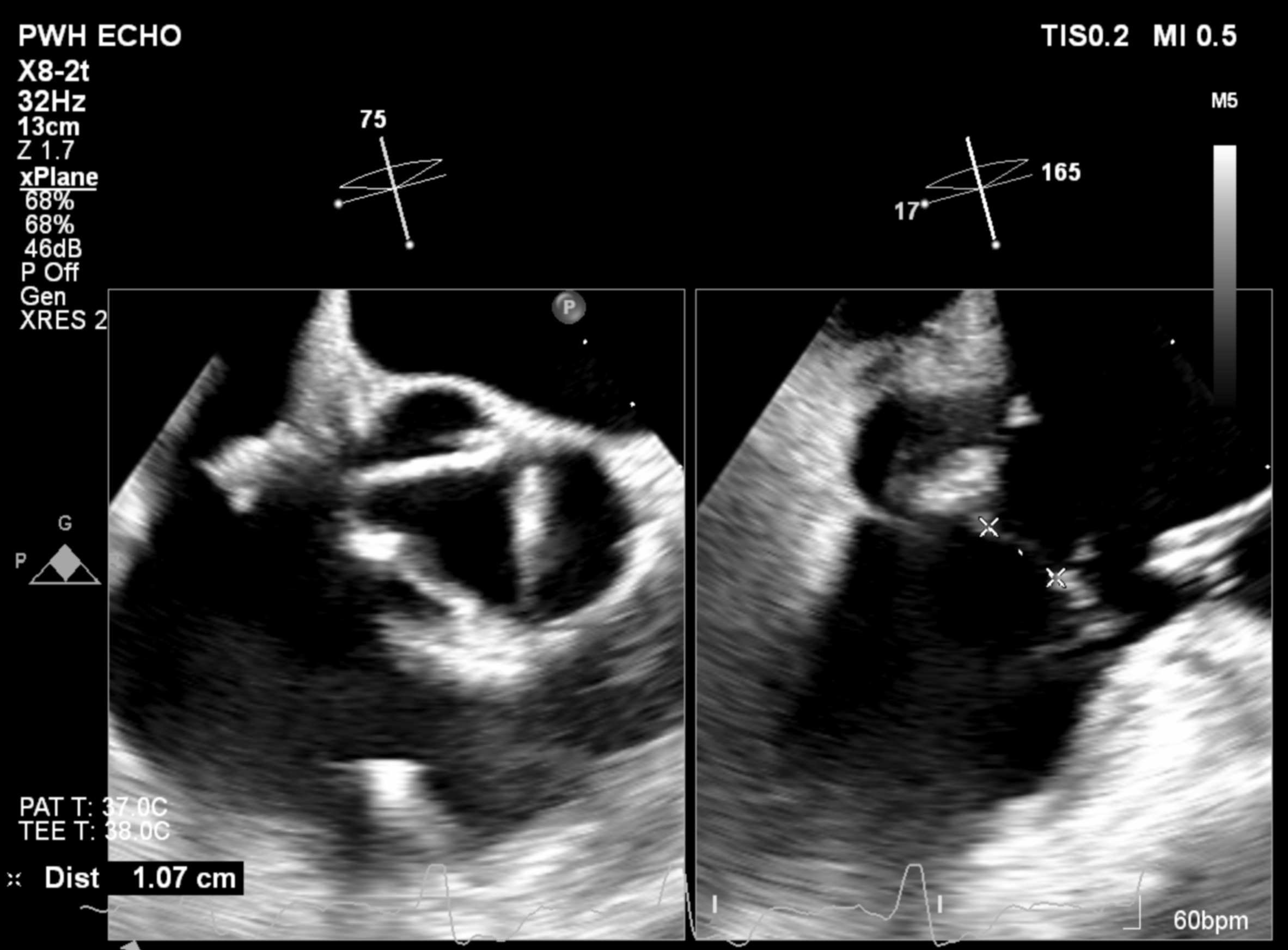
Echocardiogram showed normal biventricular systolic function. Torrential Tricuspid regurgitation with ERO 1.8cm2 and regurgitation volume 89mL. Diffuse ruptured chordae are noted at three tricuspid leaflets, an adherent tissue is found attaching to tricuspid septal leaflet. Septo-posterior gap is 1.1cm and septo-anterior gap is 1.5cm. A mobile linear mass is noted at the right atrium which suggestive of remaining tissue mass ( post extraction ).
Relevant Catheterization Findings
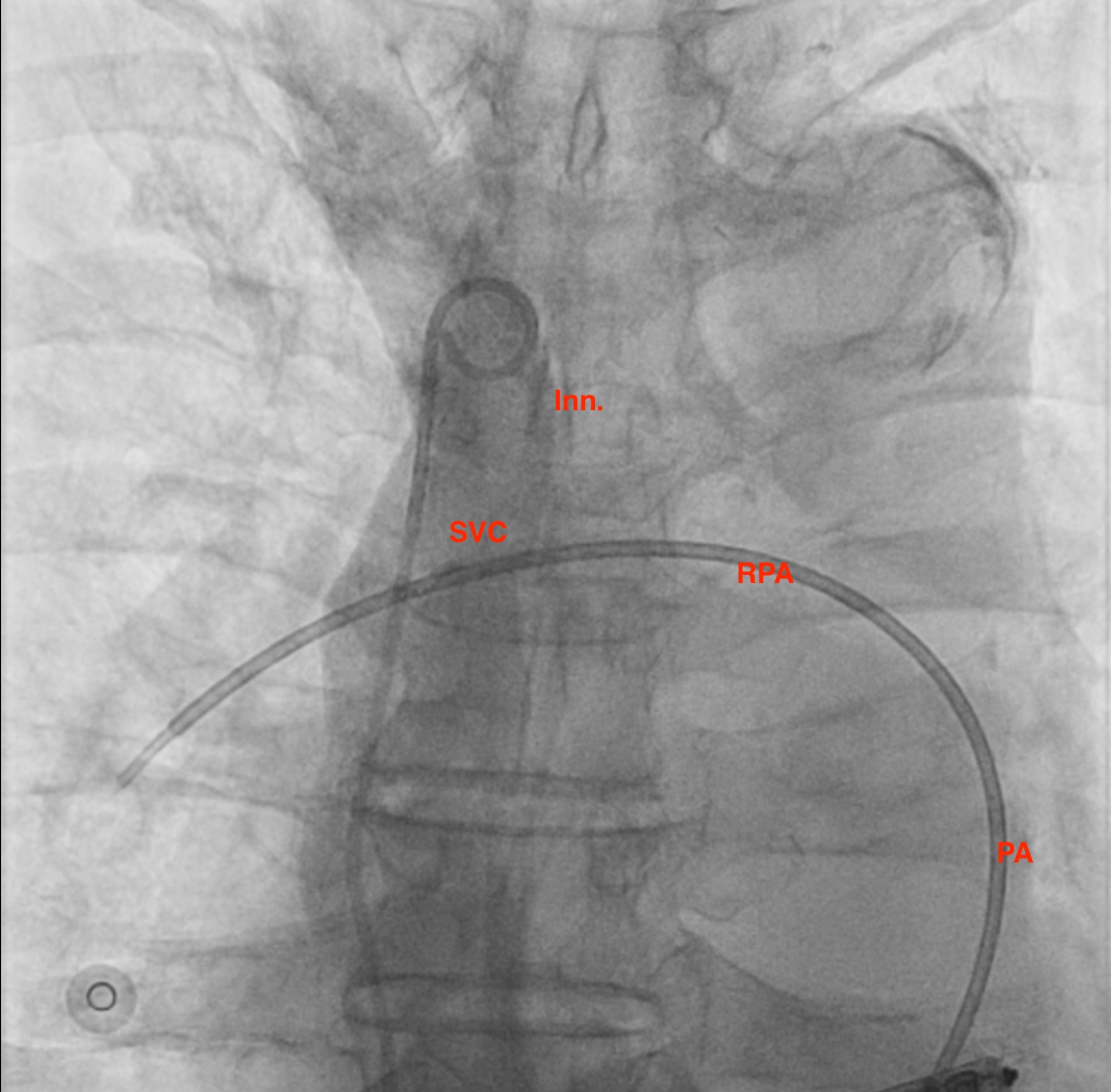
Procedure was done under local anesthesia. Bilateral femoral venous access was obtained. Right femoral vein was subsequently dilated to 24Fr for delivery of the tricvalve system. Left femoral access was used for pigtail catheter for contrast injection as landmarks in SVC and IVC before deployment of the tricvalve
Interventional Management
Procedural Step
SVC Valve and IVC Valve size were chosen according to pre procedural CT scan analysis.
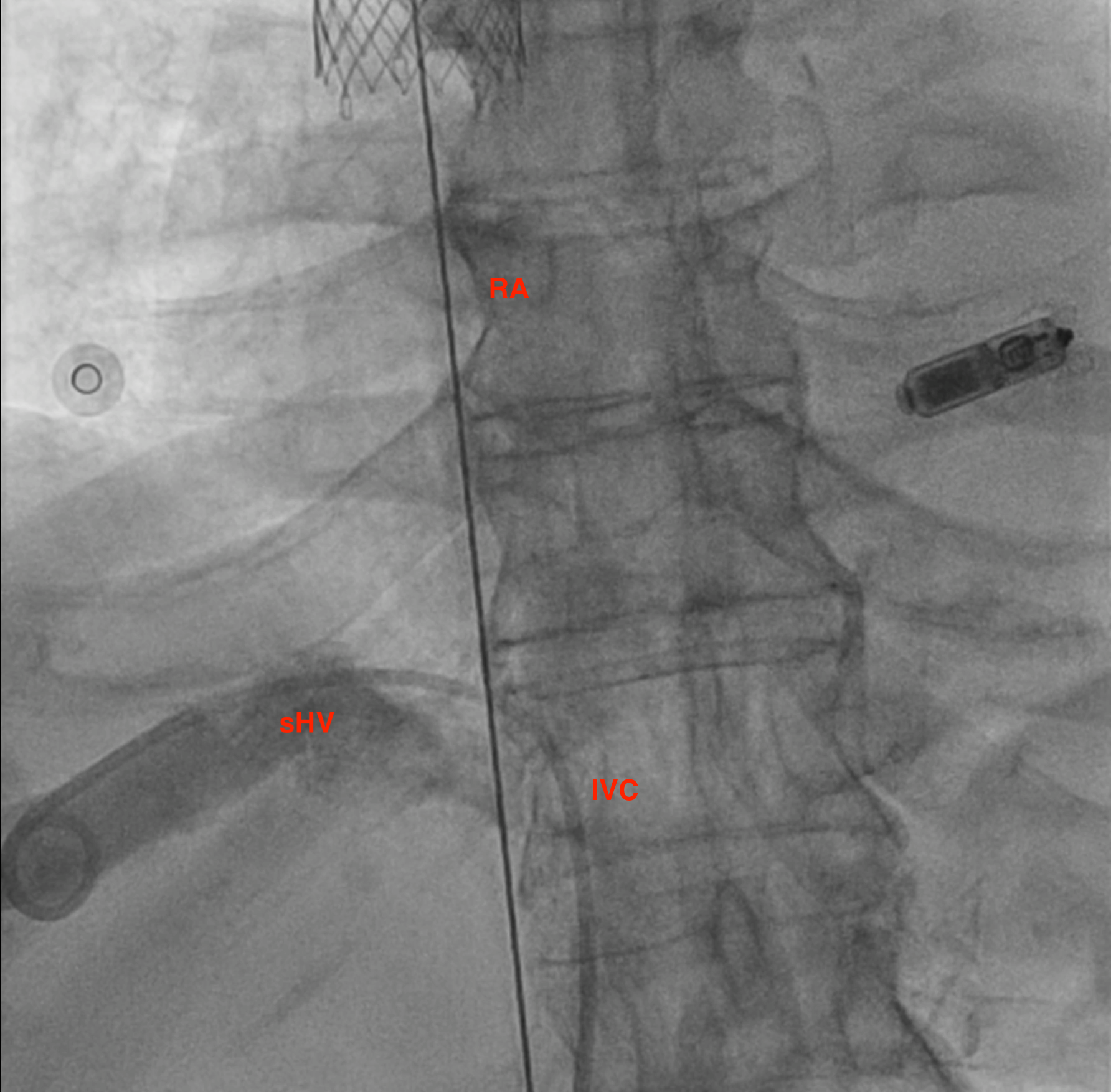
Then pigtail was introduced to the suprahepatic vein and angiogram was performed. Suprahepatic vein, IVC, and Right atrium were delineated. This time the pigtail can be staying to perform the angiogram before full deployment of the IVC valve. We aimed the skirt of the IVC valve to be above the suprahepatic vein. Again, removal of nose cone should be done carefully to avoid interaction between the valve and the system
Final angiogram in RA showed no significant leakage to SVC and IVC. Follow up echocardiogram showed disappearance of more hepatic vein reversal flow
Case Summary
The patient was able to be discharged and to cut down the use of diuretics. He suffered from right shoulder pain probably secondary to right phrenic nerve irritation. With the use of analgesics, the pain was controlled and subsided in months. His heart failure symptoms also improved to NYHA Class 1-2 and no acute heart failure admission in 9 months post implantation
Although with more data and studies regarding TEER or Orthotopic TTVR, heterotopic TTVR (eg tricvalve) still plays a role in managing some of the patients, especially challenging TV or RV anatomy or concerns underwent general anesthesia.
Although with more data and studies regarding TEER or Orthotopic TTVR, heterotopic TTVR (eg tricvalve) still plays a role in managing some of the patients, especially challenging TV or RV anatomy or concerns underwent general anesthesia.