
CASE20230806_001
Fly Me to the LA : When You Lost the Clip
By Jinho Lee, Do-Yoon Kang, Dae-Hee Kim
Presenter
Jinho Lee
Authors
Jinho Lee1, Do-Yoon Kang2, Dae-Hee Kim2
Affiliation
Kyung Hee University Medical Center, Korea (Republic of)1, Asan Medical Center, Korea (Republic of)2
Mitral Valve Intervention - TEER
Fly Me to the LA : When You Lost the Clip
Jinho Lee1, Do-Yoon Kang2, Dae-Hee Kim2
Kyung Hee University Medical Center, Korea (Republic of)1, Asan Medical Center, Korea (Republic of)2
Clinical Information
Relevant Clinical History and Physical Exam
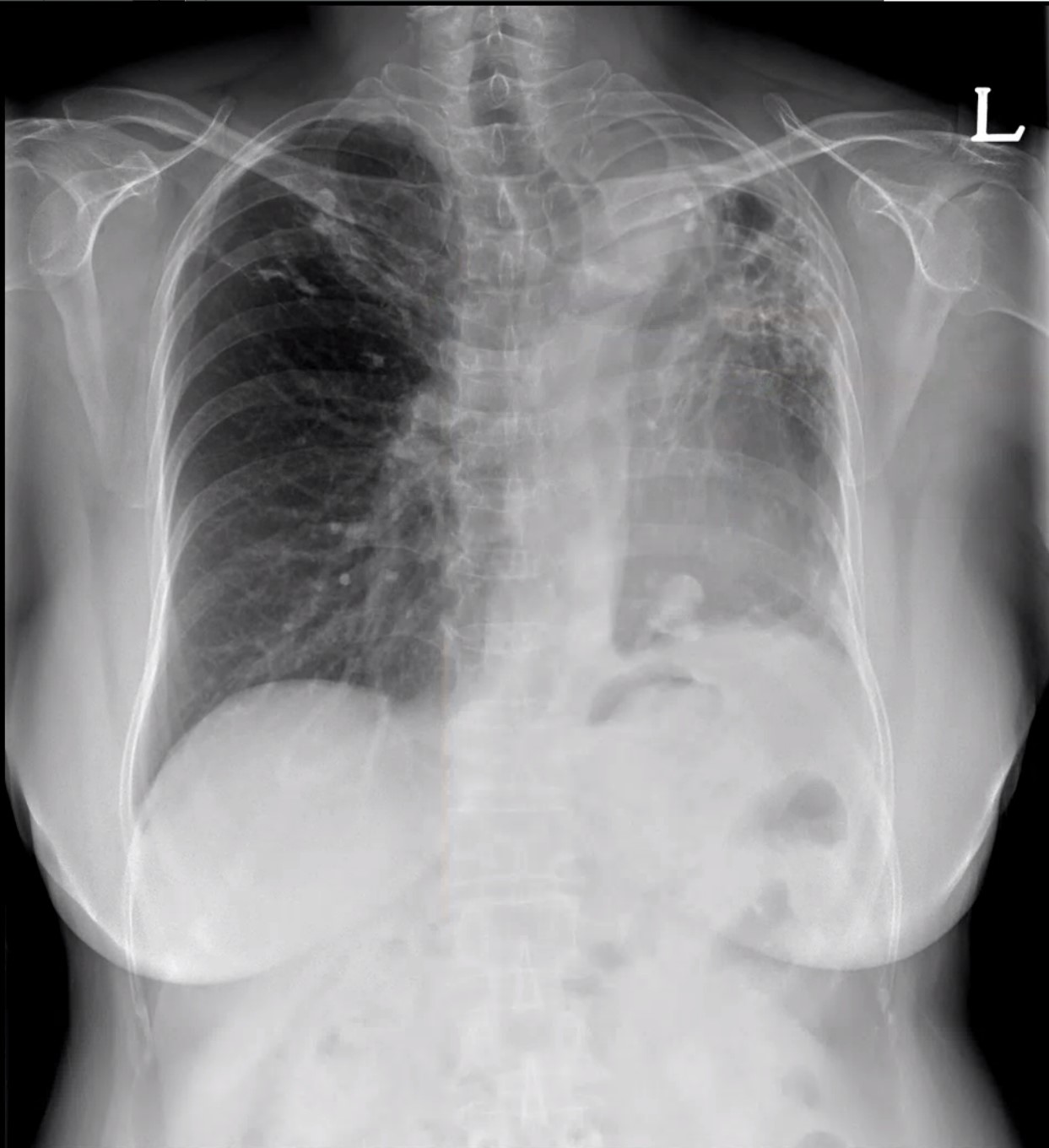
A 65-years oldfemale patient refer to hospital withsevere dyspnea. The patients had underlying disease that Tuberculosis destroyed lung, hypertension, and dyslipidemia. Intial blood pressure was 104/65mmHg with 86 beat per minute.
Relevant Test Results Prior to Catheterization
Echocardiography showed a severe eccentric mitral regurgitation (MR) due to flail motion of posterior medial scallop (P3) to medial part of middle scallop (P2) with chordae rupture. MR distal jet area was 7 cm2 , PISA radius 15 mm (at aliasing velocity of 40cm/sec) was showed in transthoracic echocardiography.
Relevant Catheterization Findings
The patient hadhigh risk of surgery which of the Society of Thoracic Surgeons (STS) risk scorecalculated a 6.5% risk of mortality due to severe lung dysfunction. After theheart team discussion, the decision was made to proceed with transcatheteredge-to-edge repair (TEER) using MitraClip G4 (Abbott, Illinois, US).
Interventional Management
Procedural Step
Under the general anesthesia, septal puncture was done at supero-posterior interatrial septum.Due to the large coaptation depth, the anatomy of the mitral valve was suitablefor MitralClip G4 XTW. Under the fluoroscopic and TEE guidance, XTW MitraClip was advancedacross the MV after transseptal puncture and deployed on the A3 and P3 scallops.In intra-operative TEE showed significant reduction of MR grade from severe tomoderate. After that, a second XT MitraClip was tried to deploy adjusted to thefirst clip and subsequent TEE demonstrated mild residual MR jets. However, inthe step of deploy, lock lines were entangled, and second clip was unclipping andunlocked. We inserted 2 shares to remove second clip, but only gripper disassembledand remnant clip flied to left atrium. Two snares were used to capture andremove the clip that was floating in the LA. However, the wings of the clipwere widely spread, making it difficult for clip enter inside to steering guidingcatheter. Moreover, passing through the inter-atrial septum was not easy. We considered convert to surgery, but fortunately,the clip finally entered the guiding catheter and passed through theinteratrial septum. With the clip captured by the snare, we removed the entireguiding catheter. After re-puncture of right femoral vein, second XTW clip was deployedadjusted to the first clip. And procedure was successfully without complications.
 003_uncliping.avi
003_uncliping.avi
005_grab_clip.avi
008_final.avi
Case Summary
In cases of clip embolization, surgery istypically required, but in this instance, the clip was successfully extractedinto the guiding catheter through prolonged snaring, avoiding the need forsurgery. Indeed, this case demonstrates the practicalfeasibility of using snaring for clip extraction in situations where clipembolization occurs. This experienceprovides valuable insights for managing similar cases in the future andhighlights the importance of careful and skilled intervention duringtranscatheter procedures to address potential complications effectively.