
CASE20230520_001
Edge-To-Edge Repair for Primary Mitral Regurgitation in a 90-Year-Old With Intractable Heart Failure
By Warit Ekprachayakoon, Anuruck Jeamanukoolkit, Wasant Soonfuang, Sukhum Tachasakunjaroen, Apinya Boonkerng
Presenter
Warit Ekprachayakoon
Authors
Warit Ekprachayakoon1, Anuruck Jeamanukoolkit1, Wasant Soonfuang1, Sukhum Tachasakunjaroen1, Apinya Boonkerng1
Affiliation
Police General Hospital, Thailand1
Mitral Valve Intervention - TEER
Edge-To-Edge Repair for Primary Mitral Regurgitation in a 90-Year-Old With Intractable Heart Failure
Warit Ekprachayakoon1, Anuruck Jeamanukoolkit1, Wasant Soonfuang1, Sukhum Tachasakunjaroen1, Apinya Boonkerng1
Police General Hospital, Thailand1
Clinical Information
Relevant Clinical History and Physical Exam
A 90-year-old woman with recent high risk NSTE-ACS underwent PCI with rotabator to RCA. She was readmitted with ADHF 3 times within 6 months. Vital signs showed a BT of 37.0 oC. BP 100/70 mmHg. PR 80 bpm. PE showed pansystolic murmur grade IV/VI at apex and fine crepitation in both lungs. She received medication for CHF. Last visit, she was admitted for staging PCI with rotabator to LAD to LM. Then she had coronary perforation at mid LAD and developed ADHF with cardiogenic shock. And on IABP.
 RPReplay_Final1684835835.mov
RPReplay_Final1684835835.mov
RPReplay_Final1684836124.mov
Relevant Test Results Prior to Catheterization
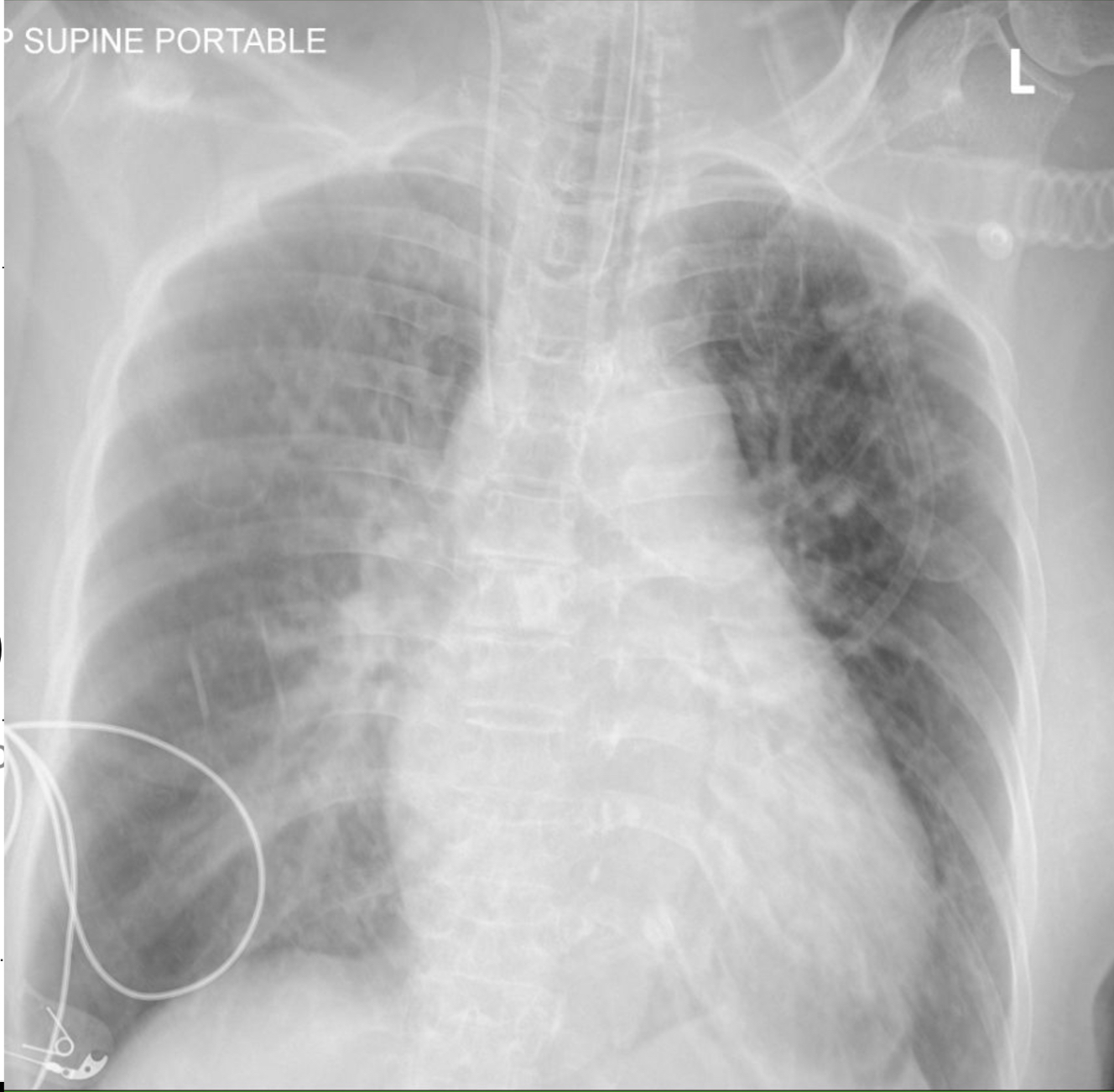
EKG showed NSR with biphasic T wave inversion at V2-V6. Chest x-ray showed perihilar congestion and cardiomegaly. Troponin T level was 163 ng/L. NT-pro BNP level was 32,000 pg/ml. An echocardiogram showed mildly reduced LV systolic function (LVEF 45%) with hypokinesia at anterior-anterolateral segments. TEE showed ruptured chordae of the flail P2 segment causing severe anterior-directed jet MR. She was diagnosed intractable congestive heart failure with severe primary MR.
RPReplay_Final1684837293.mov
RPReplay_Final1684838837.mov
Relevant Catheterization Findings
In the catheterization. Coronary artery disease was triple vessel disease. 50% stenosis at distal LM. Heavily calcification plaque at proximal to mid part of LAD with 80-90% stenosis involved DG1 bifurcation. She had 80-90% diffuse stenosis at proximal LCx and proximal to distal part of RCA. So PCI with stenting with rotator at RCA and LAD were done. After the patient developed intractable congestive heart failure. The edge-to-edge technique for mitral repair was performed
RPReplay_Final1684836688.mov
Interventional Management
Procedural Step
Under general anesthesia, a TEE probe was inserted into the mid-esophagus. A regular 0.032-inch guidewire was advanced into the SVC and an 8.5Fr Heart Span sheath long introducer was inserted through the 8 Fr femoral sheath. An 18-gauge transseptal needle was positioned within the introducer, with the needle tip remaining inside the guiding sheath.Retracting the sheath into the RA. The transseptal puncture was performed at the mid-portion and posterior aspect of the RA, access into the LA. The 8.5Fr Heart Span long introducer was further advanced into the LA over the 0.032" J-wire. Hemodynamic : PCWP was 17 mmHg. PA 35/15 mmHg (mean 22 mmHg)Subsequently, an 0.032-inch Amplatz superstiff wire was guided through the sheath and positioned within the left superior pulmonary vein. A 25Fr Abbott MitraClip delivery steerable system was then inserted and placed in the LA. The MitraClipG4 XTW was advanced through the device deployment sheaths and successfully released in the between the A2 and P2 leaflets of the mitral valve(MV). TEE showed a reduction in the severity of MR from severe to mild, with a mean MV gradient of 4 mmHg. The clip was released, and both the clip delivery system and the 25Fr introducer and sheath were removed. Hemodynamic after TEER : LAP 12 mmHg PCWP 13 mmHg PA 28/11 mmHg (mean 20 mmHg) RA 21 mmHg.Her recovery was uneventful and she was discharged on post-procedural day 5. The patient reported a marked improvement from CHF.
2023-05-23 19-29-25.mov
RPReplay_Final1684845964.mov
RPReplay_Final1684845654.mov
Case Summary
In a case of intractable heart failure accompanied by severe primary mitral regurgitation (MR), where the patient was deemed unsuitable for open surgery mitral valve replacement due to advanced age, a viable alternative treatment option was considered through transcatheter edge-to-edge repair (TEER) operation. TEER has certain limitations based on mitral valve anatomy, but in this particular patient, the location for MitraClip placement showed promise. The procedure resulted in a small atrial septal defect due to interatrial septum puncture, without significant compromise to hemodynamics. Therefore, TEER may be a more comfortable choice for high-risk surgical patients in the future.