
CASE20230519_002
The Point of No Return!
By Tanyarat Aramsareewong, Anuruck Jeamanukoolkit, Worawut Tassanawiwat, Norachai Sirisreetreerux
Presenter
Tanyarat Aramsareewong
Authors
Tanyarat Aramsareewong1, Anuruck Jeamanukoolkit2, Worawut Tassanawiwat3, Norachai Sirisreetreerux4
Affiliation
Phramongkutklao Hospital, Thailand1, Police General Hospital, Thailand2, Sunpasitthiprasong, Thailand3, Maharat Nakhonratchasima Hospital, Thailand4
TAVR - Coronary Artery Protection / Access
The Point of No Return!
Tanyarat Aramsareewong1, Anuruck Jeamanukoolkit2, Worawut Tassanawiwat3, Norachai Sirisreetreerux4
Phramongkutklao Hospital, Thailand1, Police General Hospital, Thailand2, Sunpasitthiprasong, Thailand3, Maharat Nakhonratchasima Hospital, Thailand4
Clinical Information
Relevant Clinical History and Physical Exam
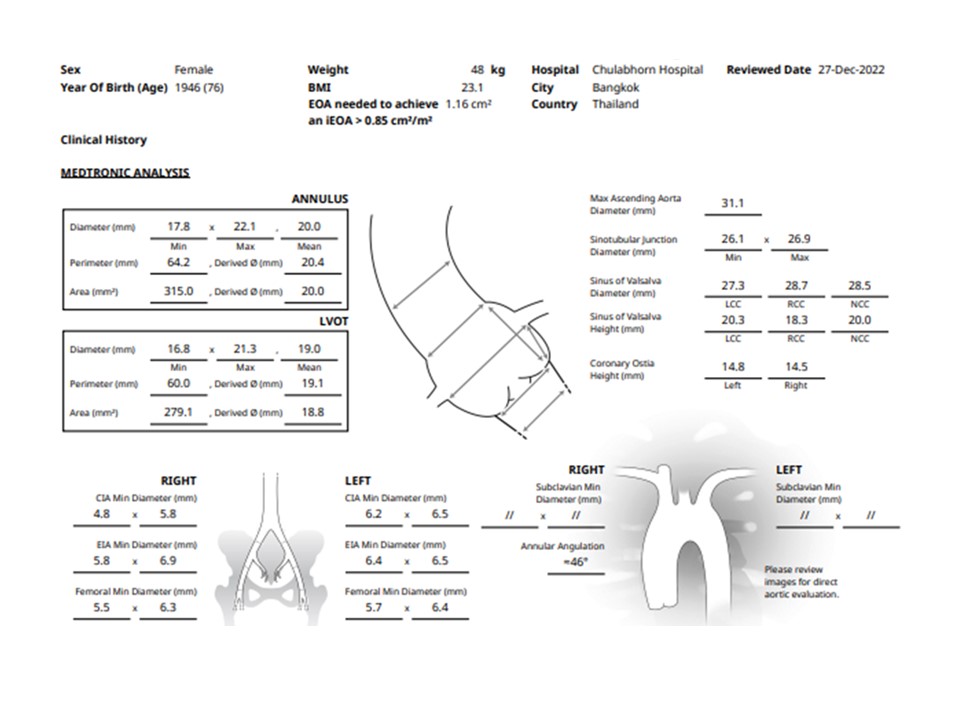
76 year-old-lady presented with history of dyspnea on exertion for 7 months. Her underlying disease was hypertension, Dyslipidemia and GERD. BW = 48 kgs, Height = 148 cm, BMI = 21.6 Kg/M2. STS score = 3.094%. Physical examination revealed severe aortic stenosis. ECG showed normal sinus rhythm with left ventricular hypertrophy. Echocardiography showed tricuspid aortic valve , severe aortic stenosis, Peak PG = 110 mmHg, Vmax = 5.25 m/sec , AVA = 0.8 cm2. No pulmonary hypertension.
 Echo.mp4
Echo.mp4
Relevant Test Results Prior to Catheterization
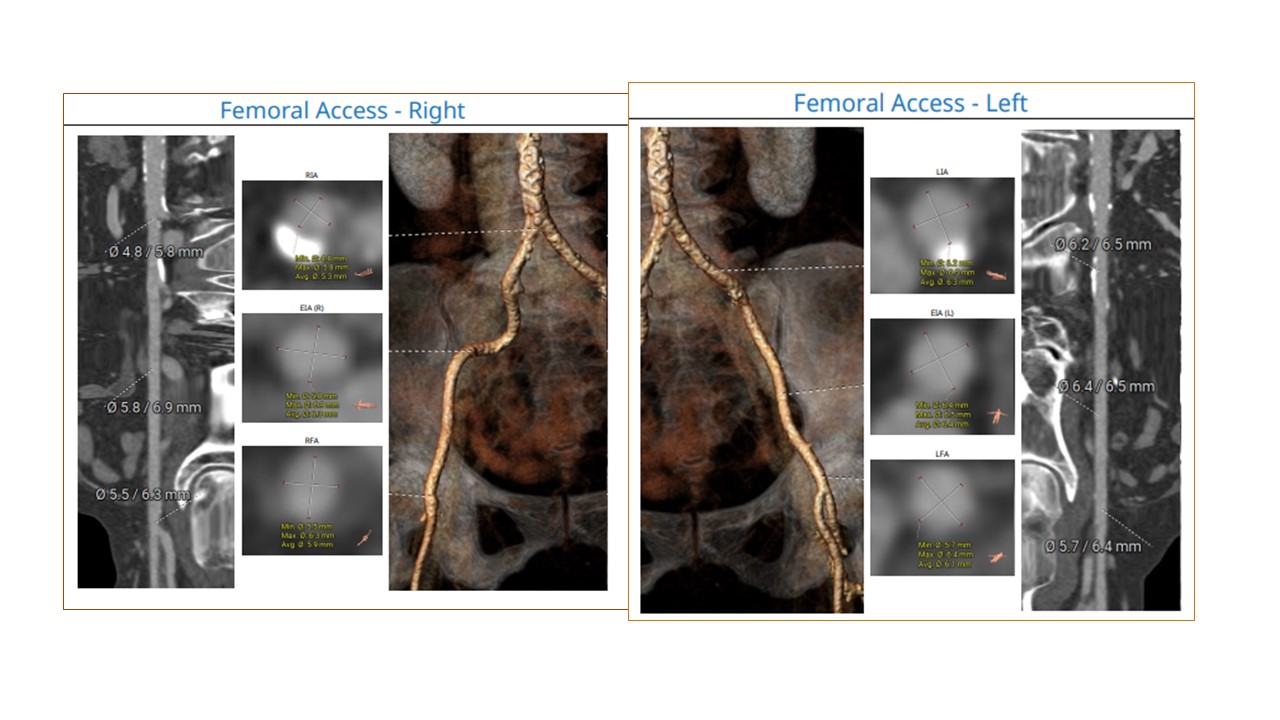
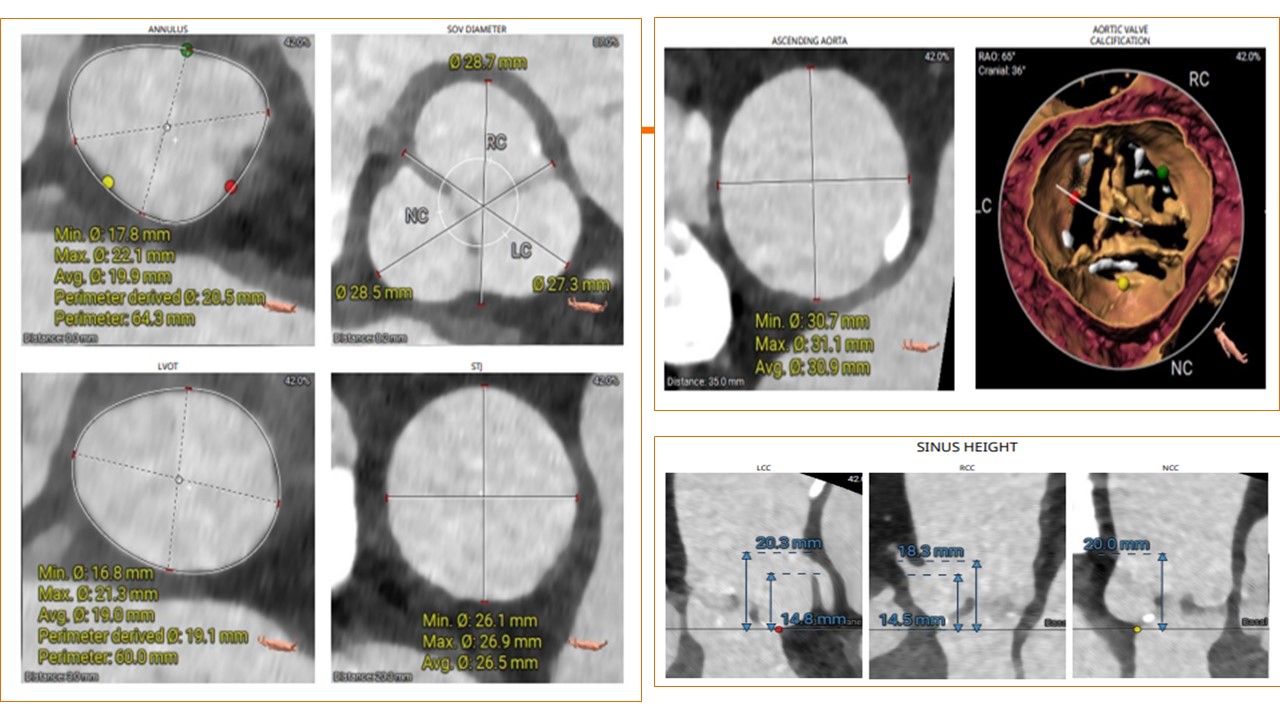
Coronary angiogram showed normal coronary artery disease. CTA whole aorta for annular sizing revealed perimeter of 64.2 mm2 ( 13% oversize for Evolut PRO 23 mm or 27% oversize for 26 mm Evolute PRO )
procedure.mp4
Relevant Catheterization Findings
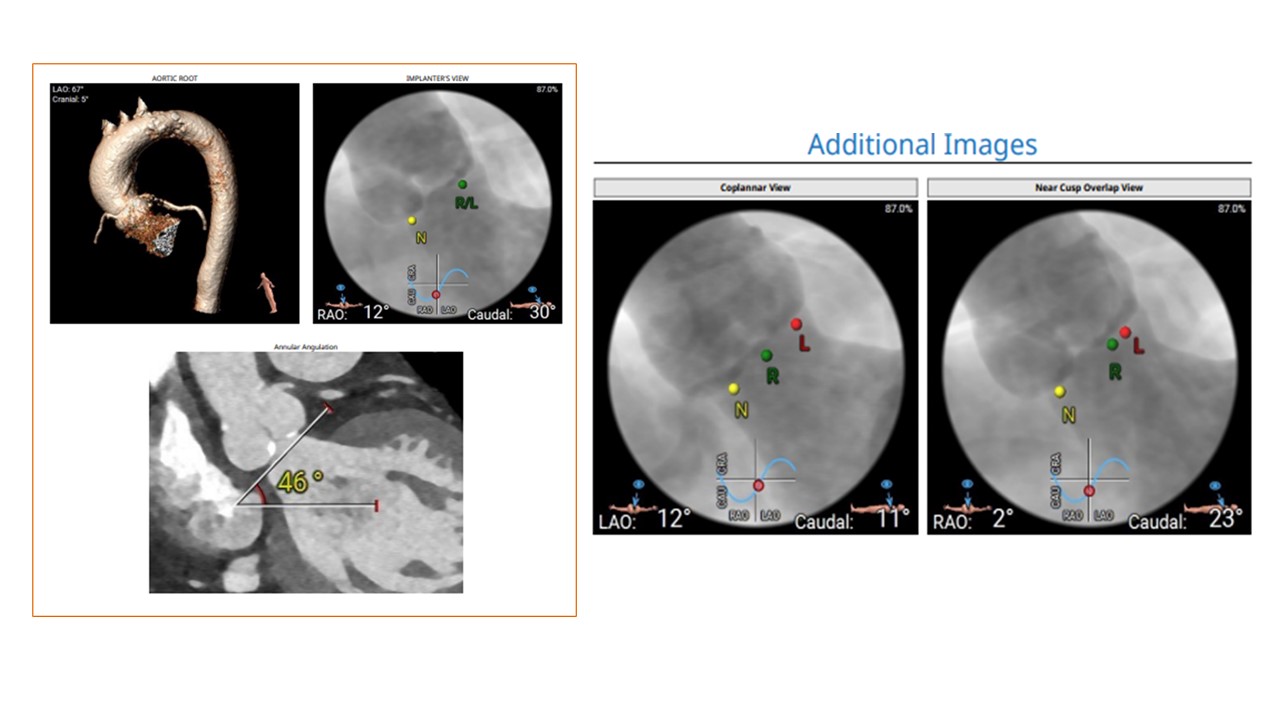
The left heart catheterization was performed before the procedure which confirmed significant peak to peak pressure gradient of 65 mmHg. The pre-procedure angiogram to confirmed cusp-overlap view which revealed mild aortic regurgitation.
Presentation5.mp4
Interventional Management
Procedural Step
The planning for the procedure was meticulously carried out by the heart team, utilizing the 26 mm Evolute Pro+ valve. The operator intended to implant the valve at a higher position due to a 27% oversizing of the valve.The valve was implanted without pre-dilatation, resulting in an excessively high implantation depth. Recognizing the error, the valve was incidentally moved upwards. Then the operator's attempts to recapture the valve unfortunaly the deployment reached a point of no return, causing deformation of both the valve and the capsule.To address this unforeseen complication, the operator decided to retrieve the deformed valve back to the ascending aorta. This was achieved by employing a 20 French delivery sheath to recapture the deformed valve. Subsequently, the deformed valve was successfully removed through the right femoral artery. A new 23 mm Evolute Pro+ valve was then skillfully implanted, achieving a final implantation depth of 3 mm.Post-procedure, an angiogram was performed, revealing a trivial aortic regurgitation and a residual gradient of 3 mm. Unfortunately, the retrieval of the deformed valve resulted in an injury to the right common femoral artery. However, effective hemostasis of the right common femoral artery was achieved by employing a prolonged balloon inflation cross-over via the left femoral artery, in conjunction with external compression using an absorbable hemostatic gelatin sponge.
Case Summary
1. Effective communication among the heart team is utmost importance, particularly during critical moments, to ensure smooth coordination and optimal patient outcomes. 2. Retrieval of a 23 mm self-expandable valve through a 20 French sheath has been demonstrated as a safe and feasible procedure. resulting in minimal femoral artery injury. 3. The application of an absorbable hemostatic gelatin sponge, combined with external vessel compression and prolong intra-vessel balloon dilatation, represents a potential novel technique to repair vessels and potentially avoid the need for surgical consultation.