
CASE20230511_002
A Case of TAVR Treatment for Bioprosthetic Aortic Valve Dysfunction
By Wenduo Zhang
Presenter
Wenduo Zhang
Authors
Wenduo Zhang1
Affiliation
Beijing Hospital, China1
TAVR - Valve-in-Valve TAVR
A Case of TAVR Treatment for Bioprosthetic Aortic Valve Dysfunction
Wenduo Zhang1
Beijing Hospital, China1
Clinical Information
Relevant Clinical History and Physical Exam
The patient, male, 80 years old, underwent aortic valve replacement in 2014 due to the surgical operation of severe aortic stenosis due to rheumatic heart disease. In this year, after walking 500 meters, he felt chest tightness and suffocation, and rest could improve. He had a history of hypertension for 40 years. Grade III-IV/6 systolic murmur can be heard in the auscultation area of aortic valve.
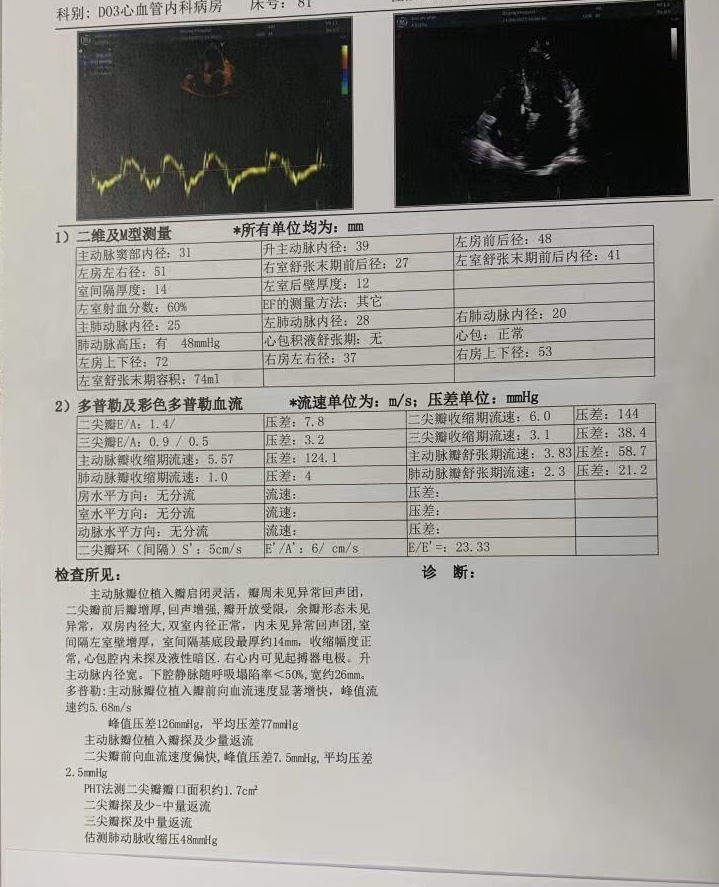
Relevant Test Results Prior to Catheterization
Mean Gradient 77mmHg Peak Velocity 5.68m/s EF 60%LVEDD 41mm
Relevant Catheterization Findings
Coronary angiography with normal coronary artery
Interventional Management
Procedural Step
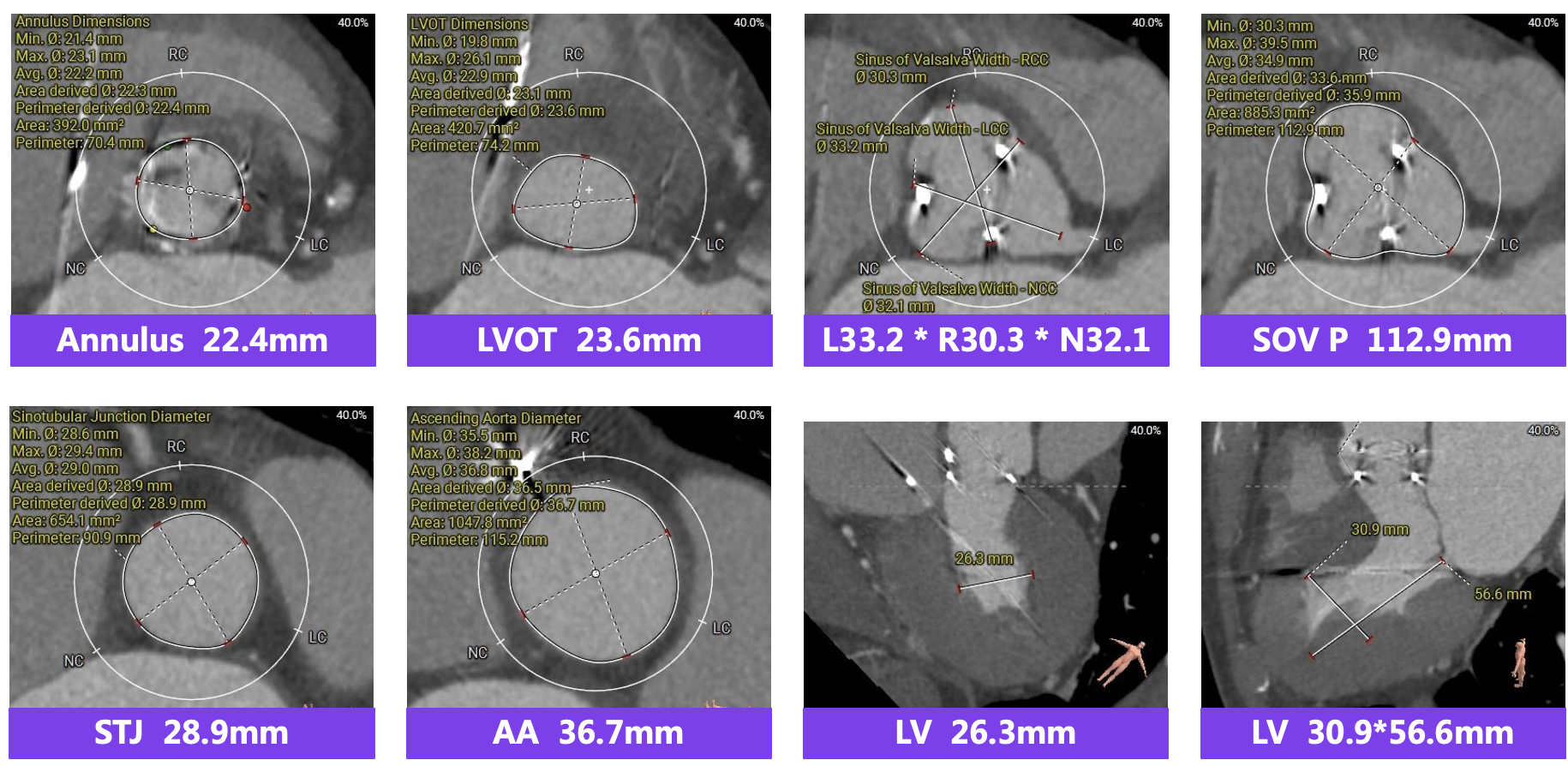
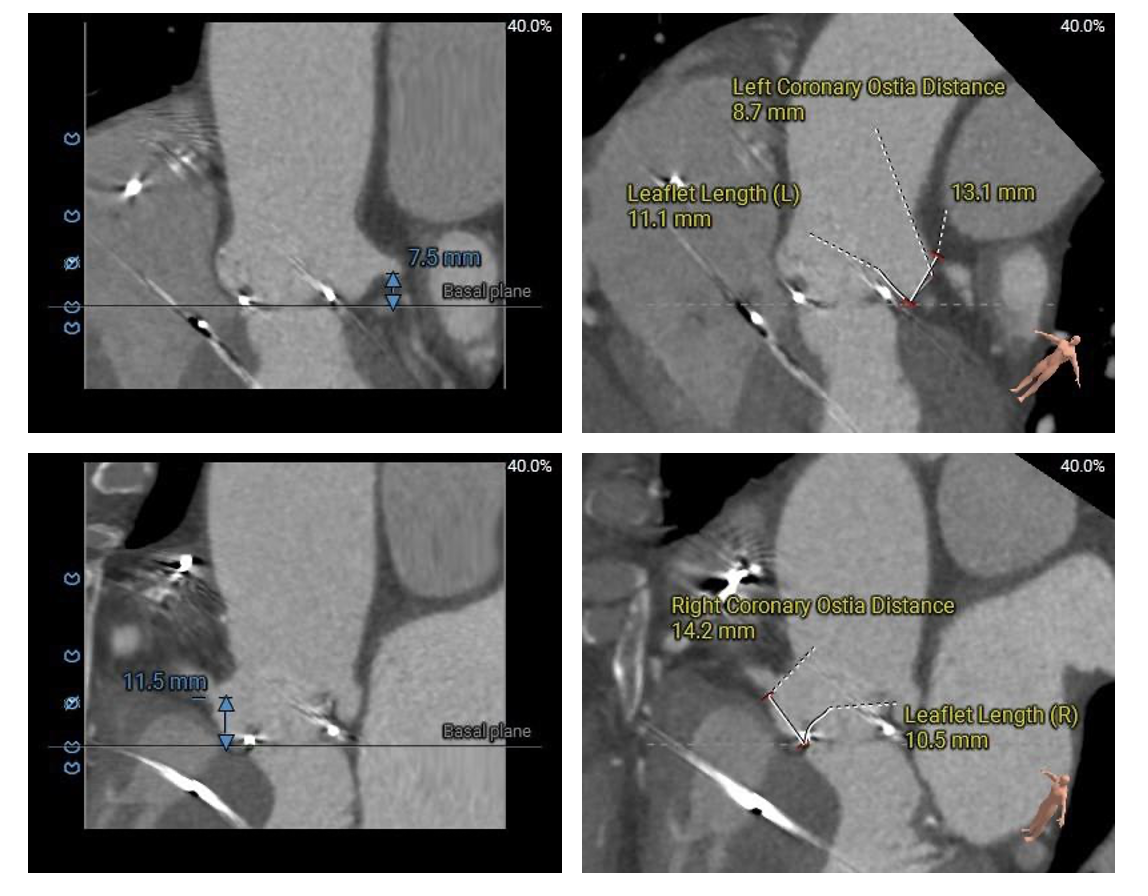
In the case of biological valve failure, the original biological valve is relatively small, and the estimated valve shape has a significant impact. The anchoring is acceptable, and there is a certain risk of decline during the release process. It is expected that the TaurusElite AV23 valve will be implanted through the right femoral main approach without pre dilation, with initial positioning at 0 position. After the valve is released to the working position, the valve position and shape will be fully evaluated in multiple positions. Based on the ultrasound results, it will be confirmed that there is no error before release. In the first four times, the valve has slipped a lot, and a replacement position will be considered, After multi angle adjustment, it was found that the central position of the right sinus was still better for rapid pacing release to the working position, with a multi angle contrast ratio of about 8mm. Ultrasound showed no significant limitation of the mitral valve, and the hemodynamic results were satisfactory. Considering the possibility of the valve frame moving down again from the coaxial axis, it was decided to release to the extreme recovery position to observe the valve frame moving down
 first .mp4
first .mp4
valve release.mp4
final angio.mp4
Case Summary
Selection and adjustment of projection angle, with the bottom of the sheath tube flush with the artificial valve frame, reaching the pre release position;Recommend ± 2mm between the bottom of the valve holder and the plane of the virtual valve ring as the initial release position, and use the recyclable function to try the best anchoring point; Slowly release and anchor with adjacent tissues, quickly release to the valve working position ,and choose different pacing strategies based on the patient's condition;Ultrasound or DSA (multi section, multi angle) CALM principles are used to evaluate the position, morphology, coaxiality, and functional adjacent tissue effects of artificial valves.