
CASE20230508_001
High-Risk PCI With Rotatripsy and TAVR With Extracorporeal Membrane Oxygenation Support: A Case Report
By Huan-Chiu Lin, Tien Ping Tsao, Yung-Tsai Lee, Wei-Hsian Yin
Presenter
Huan-Chiu Lin
Authors
Huan-Chiu Lin1, Tien Ping Tsao1, Yung-Tsai Lee1, Wei-Hsian Yin1
Affiliation
Cheng Hsin General Hospital, Taiwan1
TAVR - Complex TAVR
High-Risk PCI With Rotatripsy and TAVR With Extracorporeal Membrane Oxygenation Support: A Case Report
Huan-Chiu Lin1, Tien Ping Tsao1, Yung-Tsai Lee1, Wei-Hsian Yin1
Cheng Hsin General Hospital, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
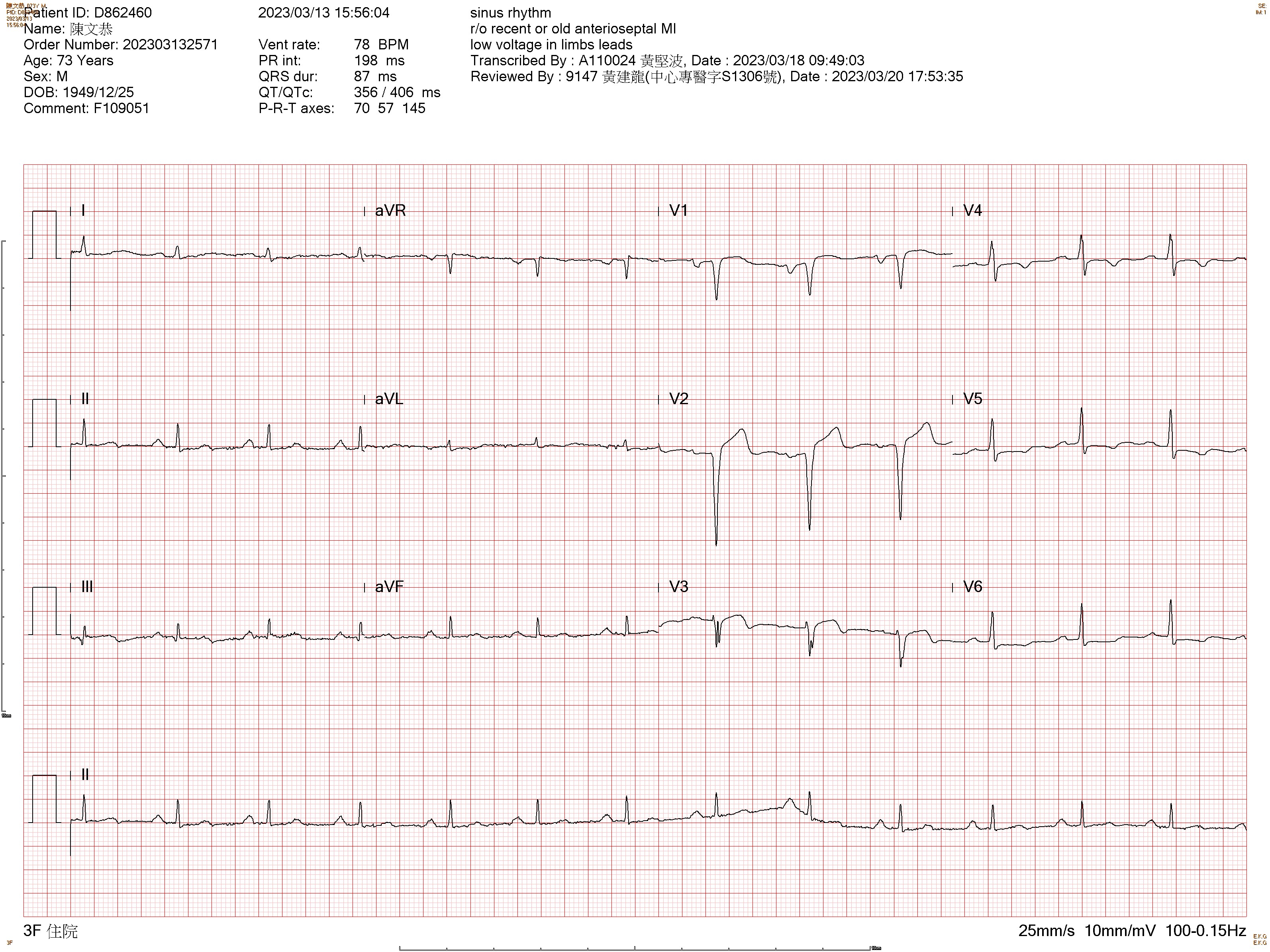
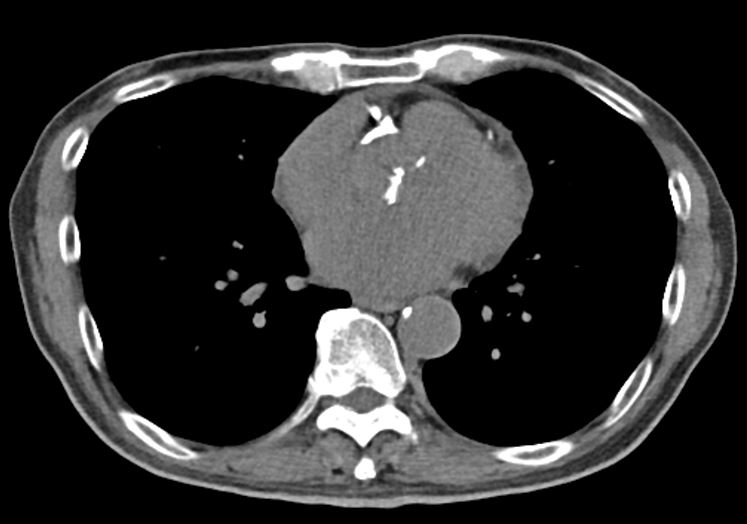
This 74-year-old male with a history of type 2 diabetes mellitus for 20+ years under regular medical treatment. He complained of intermitted chest distress with dyspnea recently. He came to our outpatient clinic for evaluation. Physical examination revealed Grade IV systolic murmur over the right upper sternum border. ECG showed recent anteroseptal wall myocardial infarction. A previous CT scan at another hospital revealed severe coro

Relevant Test Results Prior to Catheterization
Lab data showed stage 2 chronic kidney disease, with a normal range of liver function test results. Echocardiogram showed severe LV systolic dysfunction, LVEF 18%, and severe low flow-low gradient aortic stenosis, moderate-severe mitral regurgitation, and moderate tricuspid regurgitation, and estimated pulmonary artery pressure is 45mmHg.
 D862460-PRE-4C.mp4
D862460-PRE-4C.mp4
D862460- OP-AS.mp4
D862460- OP-AS-COLOR.mp4
Relevant Catheterization Findings
Coronary angiography showed left main ostium to middle portion of left anterior descending coronary artery long diffuse lesion with heavy calcification. There was a huge calcium nodule at ostium of right coronary artery, with 90% stenosis. Left main and triple vessel disease was diagnosed, complicated with heavy calcification.
D862460_006.AVI
D862460_007.AVI
D862460_011.AVI
Interventional Management
Procedural Step
1.Before the procedure, ECMO was inserted via right femoral artery and vein for periprocedural hemodynamic support. 2.LMCA was engaged with EBU3.5/6F(SH), and wired Pilot 50 to LAD-D.3.IVUS and Finecross microcatheter were both failed to cross the LAD-P lesion.4.Rotational atherectomy was performed with 1.25mm burr at 180,000 rpm.5.IVUS showed diffuse atherosclerotic plaque with moderate-severe superficial calcium(around 270 degrees of calcium arc) from LAD-M to LAD-P, and RVD is 2.5mm at LAD-M, 3.0-3.5mm at LAD-P, and 4.0mm at LM.6.Because of heavy calcification, a 2.5 x 12mm IVL Shockwave balloon was delivered to LAD-M, inflated at 4atm to facilitate sonic pressure wave emission for calcium modification, and the lesions were dilated successfully after then.7.Deployed a 2.25 x 32mm Synergy XD DES at LAD-M, and a 2.75 x 38mm Synergy XD DES from LAD-M to LM at 14atm.8.RCA was engaged with JR/6F(SH), and wired Pilot 50 to RCA-D.9.IVUS and Finecross microcatheter were both failed to cross the RCA-P lesion.10.Rotational atherectomy was performed with 1.5mm burr at 180,000 rpm.11.IVUS showed which revealed a huge calcium nodule at RCA-ostium, partial break after previous lithotripsy and balloon dilatation, and RVD is 4.0mm12.Deployed a 3.5 x 16mm Synergy XD DES at 12-16atm.13.For LFLG AS, a 26mm Edwards Sapien 3 valve was deployed successfully.14.TEE showed optimal result with 5mmHg for mean pressure gradient, and mild paravalvular leakage.
D862460_022.AVI
D862460_125.AVI
D862460_170.AVI
Case Summary
It is better to start up front, especially when an MCS device, like ECMO, requires time to institute, it is very difficult to stop in the middle of the procedure on a patient who is going to shock. If a patient is hemodynamically stable post-procedure, the device can usually be removed immediately. Early initiation of MCS can mitigate the consequences of hypoperfusion, worsening ischemia, and declining cardiac function. High-risk PCI and simultaneous TAVR is teamwork, including shared decision-making, the success of the procedure and good clinical outcome depends on the whole team's cooperation. The combination of RotaTripsy may be useful in the treatment of severely calcified lesions.