
CASE20230506_002
A Successful Transcatheter Aortic Valve Implantation of Venus A-Plus in Functional Bicuspid Aortic Valve With Large Annulus
By Yi Xu, Zicheng Li
Presenter
Yi Xu
Authors
Yi Xu1, Zicheng Li2
Affiliation
The First Affiliated Hospital of Jinan University, China1, First Affiliated Hospital of Ji'Nan University, China2
TAVR - Bicuspid AV
A Successful Transcatheter Aortic Valve Implantation of Venus A-Plus in Functional Bicuspid Aortic Valve With Large Annulus
Yi Xu1, Zicheng Li2
The First Affiliated Hospital of Jinan University, China1, First Affiliated Hospital of Ji'Nan University, China2
Clinical Information
Relevant Clinical History and Physical Exam
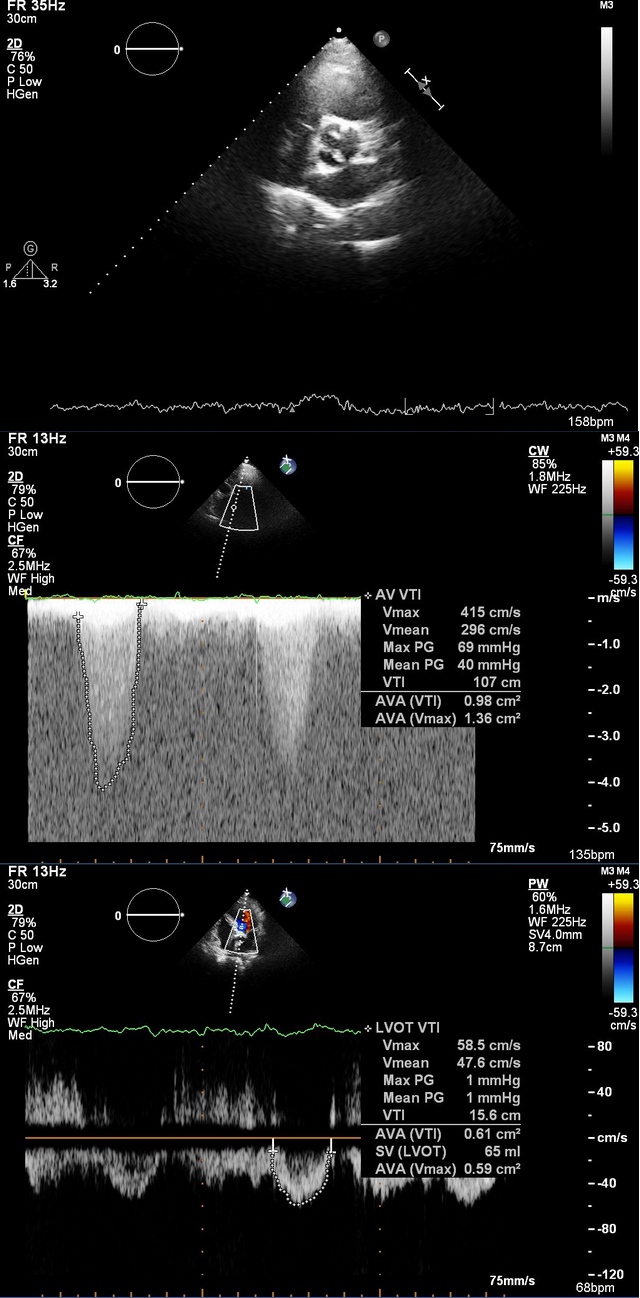
A 76-year-old male wasadmitted to our hospital due to recurrent chest tightness for 1 year, worsenedfor 1 month. His comorbidities include hypertension and Parkinson'sdisease. Grade 4 systolic murmur in the left 2nd intercostal space could beheard. Echocardiogram showed severe aortic stenosis with mild to severe aorticregurgitation (Vmax: 5.85m/s, MPG: 40mmHg, AVA: 0.61 cm2, ARA: 6.6cm2) and normal systolic function (LVEF:55%).
Relevant Test Results Prior to Catheterization
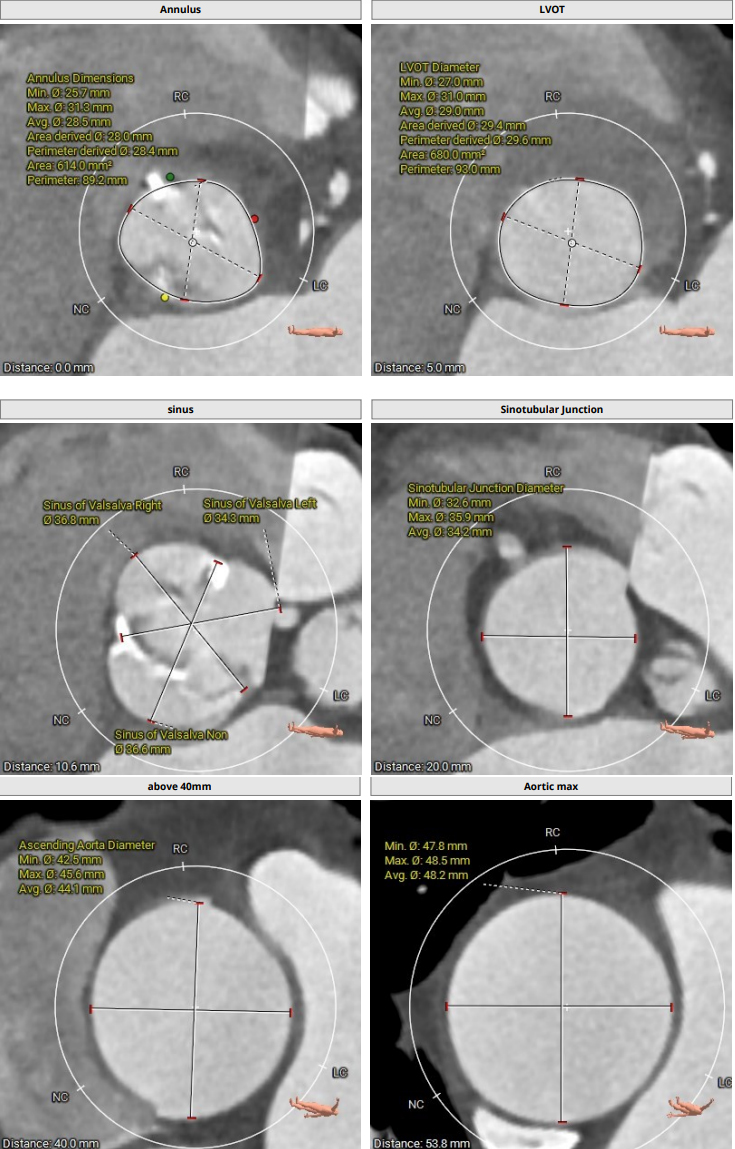
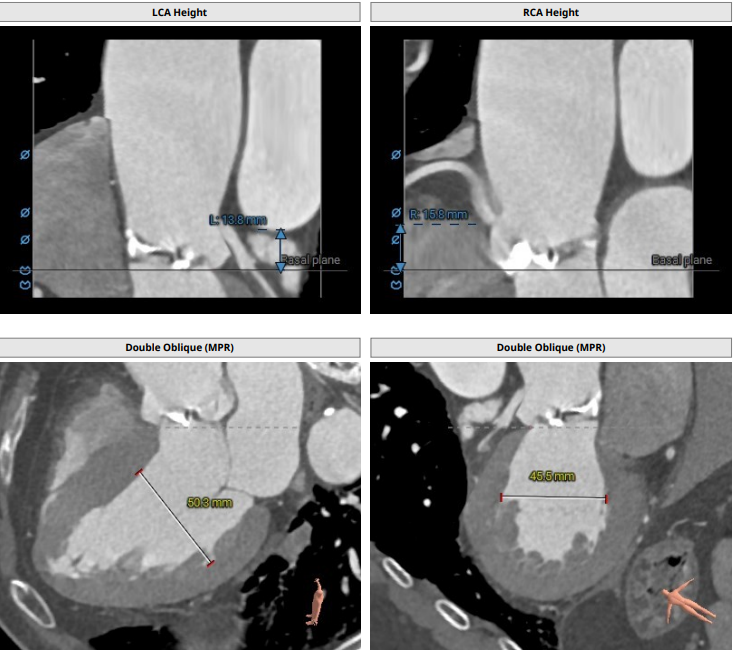
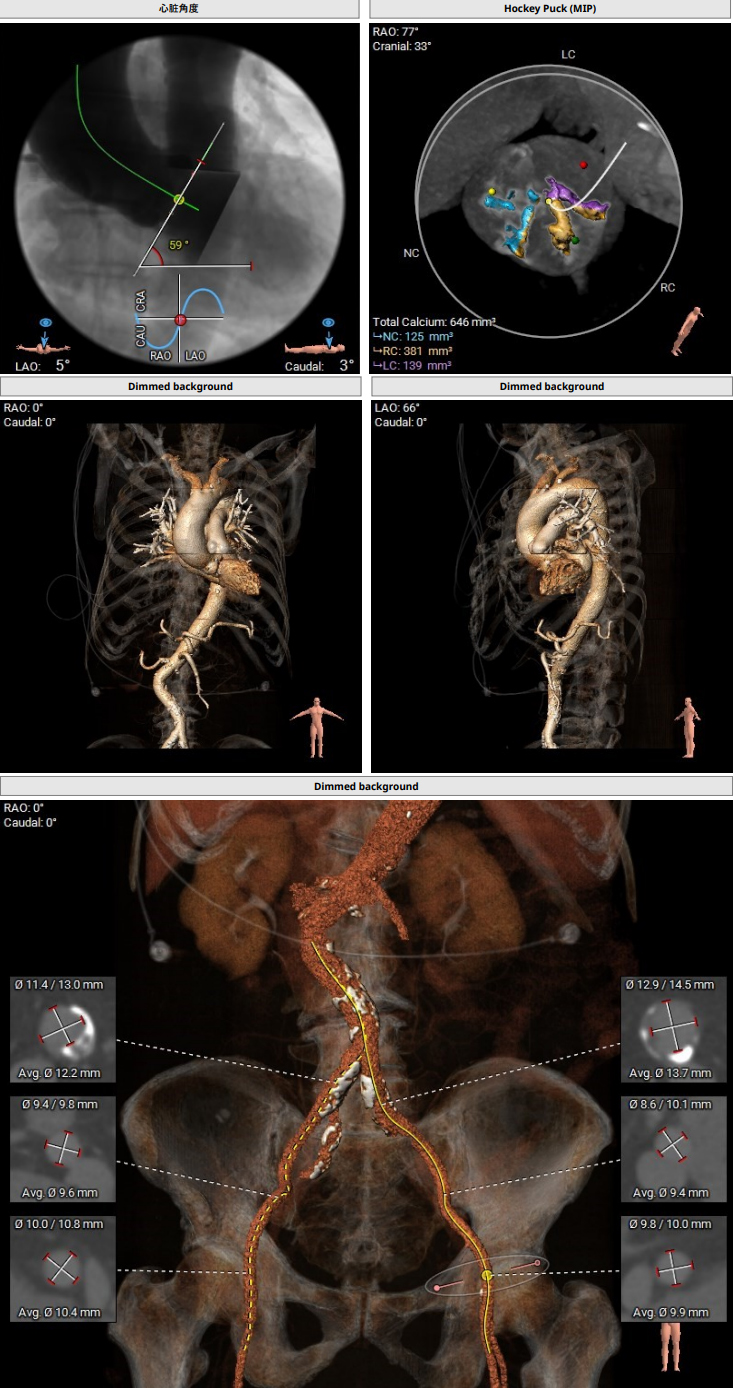
Pre-operative CTshowed a functional bicuspid aortic valve with the left and right leafletsfused. The valve was severely calcified. The mean aortic annulus diameter was28.0mm and the perimeter was 89.2mm, with an area of 614.0 mm2. The sinus of Valsalva diameter was 34.3, 36.8, and36.6 mm for the left, right, and noncoronary cusps, respectively. Coronaryheights were 13.8mm (left) and 15.8mm (right). Ascending aorta wasdilated (maximum diameter 44.1mm). The heart angle was 59°.
Relevant Catheterization Findings
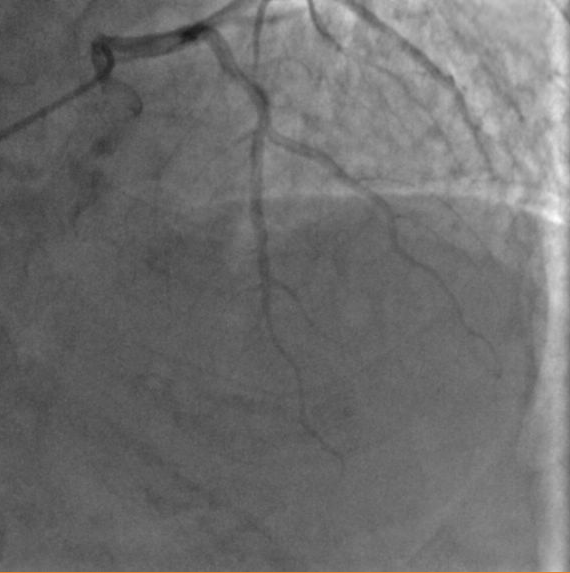
Coronary angiographyshowed a 40% stenosis in distal LAD and no other significant stenosis.

Interventional Management
Procedural Step
The procedure wasconducted under general anathesia. Left femoral artery puncture was obtained and a6-Fr sheath was placed. Right femoral artery was punctured underangio-guidance and another 6-Fr sheath was placed. The right 6-Fr sheath wasthen replaced by a 10-Fr one. Temporary pacing wire was placed through leftfemoral vein. Angiogram performed at the aortic root showing good leafletmobility. The coronary arteries were also showed well. An AL2 diagnosticcatheter was sent to the ascending aortavia right femoral artery. The aorticvalve was crossed with wire under guidance of the AL2 catheter. A PIG catheterwas exchanged and basal pressures were measured (LV pressure 170mmHg, aorticpressure 110mmHg). The 10-Fr sheath was replaced by a 20-Fr sheath. Aortic valvuloplasty was done using 23mm balloon. A L29 Venus-A-Plus self-expandable valve (Venus Medtech, Hangzhou, China) was loaded,positioned, and deployed under rapid ventricular pacing. LV and aortic pressureswere measured again, showing 120mmHg both. Aortic root angiogram was alsorepeated, showing good placementof the prosthesis with minimal regurgitation.The expansion was not satisfying, thus a post-dilatation was performed with23mm balloon. Post-procedural echo showed well-functioning valve with no signsof regurgitation. ECG monitorshowed no newly onset of heart block. The patientrecovered well and was discharged 4 days after the procedure.
 case videos 1.avi
case videos 1.avi
case videos 2.avi
case videos 3.avi
Case Summary
Bicuspid aortic valves often come along withlarge annulus, heavy calcification, and dilated ascending aorta. which lead to higherrates of worse outcomes and failure of TAVI. Here we report a case offunctional bicuspid aortic valve with annular perimeter of 89.2mm. The procedurewas successful with a L29 Venus A-Plus valve implanted. Detailed pre-operative echoand CT evaluation, the choice of optimal self-expandable valve and angiographicpositions, as well as careful techniqes during procedure help to achieve asatisfying result in this patient. Our case adds more evidence to support theuse of Venus-A-Plus self-expandable valve inpatients with bicuspid aortic valves and large annuli.