
CASE20220611_002
Combined antegrade and retrograde percutaneous closure of perimitral pseudoaneurysm causing paravalvular leakage after mitral valve surgery
By Krissada Meemook, Pornpimol Vichitchaisilp
Presenter
Pornpimol Vichitchaisilp
Authors
Krissada Meemook1, Pornpimol Vichitchaisilp1
Affiliation
Ramathibodi Hospital, Thailand1
Valve - Others (Valve)
Combined antegrade and retrograde percutaneous closure of perimitral pseudoaneurysm causing paravalvular leakage after mitral valve surgery
Krissada Meemook1, Pornpimol Vichitchaisilp1
Ramathibodi Hospital, Thailand1
Clinical Information
Relevant Clinical History and Physical Exam
An 83-year-old male with status 5 years post pacemaker implantation due to atrial fibrillation and postoperative complete heart block following minimally invasive mitral valve replacement and tricuspid valve repair, presented at our hospital with dyspnea on exertion. He was consulted by a CVT surgeon for evaluation and treatment of recurrent postoperative severe mitral regurgitation. His physical examination revealed normotension with a pansystolic murmur at the apical area.
Relevant Test Results Prior to Catheterization
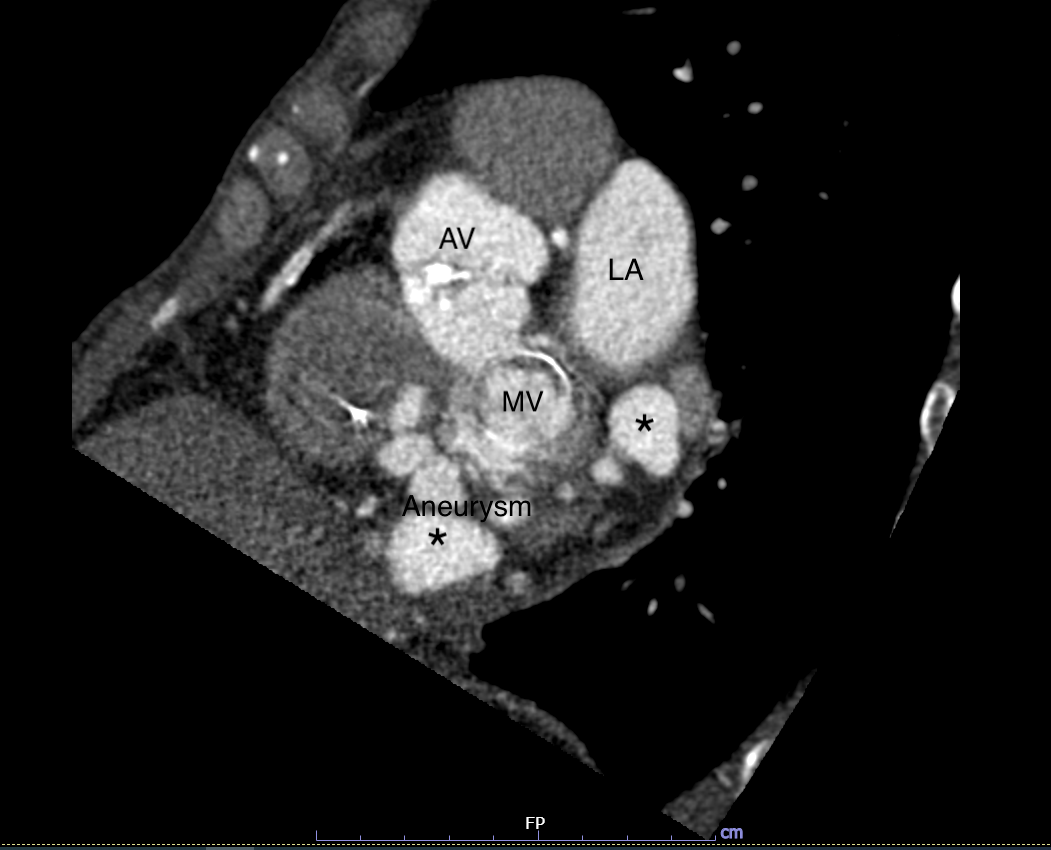
The echocardiogram showed well-seated MV bioprosthesis. There was complex paravalvular regurgitation (PVL) beneath the MV at medial side of left ventricle (LV). The flow directed toward the aneurysmal sac and continued to left atrium (LA). Another smaller PVL with aneurysm was found at lateral side of LV between the LA and LV.
 TEE1.mp4
TEE1.mp4
TEE2.mp4
Relevant Catheterization Findings
Combined right and left heart catheterization was performed, showing multiple submitral outpouching lesions with some extravasation of contrast into LA. The left ventricle end diastolic pressure was 7 mmHg. The mean pulmonary arterial pressure was 13 mmHg with no step-up in oxygen saturation. The coronary angiogram was normal.
LV gram 1.mp4
LV gram 2.mp4
Interventional Management
Procedural Step
Given his age, frailty and previous thoracic surgery, the patient was deemed to be at high risk for surgical closure. Therefore, a decision to perform percutaneous pseudoaneurysm closure was made.
Antegrade.mp4
Retrograde.mp4
LV gram.mp4
Case Summary
Percutaneous left ventricular pseudoaneurysm closure might be a challenging and feasible therapeutic option for high-risk surgical candidates. There is no standardized approach for left ventricular pseudoaneurysm closure. The use of multimodality imaging and proper pre-procedural planning are the key to success.