
CASE20220606_001
Transcatheter tricuspid valve-in-ring and large submitral LV pseudoaneurysm closure with Amplatzer vascular plug II in a post-operative patient with pacemaker lead
By Thinnakrit Sasiprapha, Krissada Meemook, Mann Chandavimol, Tawai Ngernsritrakul
Presenter
Thinnakrit Sasiprapha
Authors
Thinnakrit Sasiprapha1, Krissada Meemook2, Mann Chandavimol1, Tawai Ngernsritrakul1
Affiliation
Ramathibodi Hospital, Thailand1, Ramathibodi Hospital Mahidol University, Thailand2
Structural Heart Disease - Others (Structural Heart Disease)
Transcatheter tricuspid valve-in-ring and large submitral LV pseudoaneurysm closure with Amplatzer vascular plug II in a post-operative patient with pacemaker lead
Thinnakrit Sasiprapha1, Krissada Meemook2, Mann Chandavimol1, Tawai Ngernsritrakul1
Ramathibodi Hospital, Thailand1, Ramathibodi Hospital Mahidol University, Thailand2
Clinical Information
Patient initials or Identifier Number
WS
Relevant Clinical History and Physical Exam
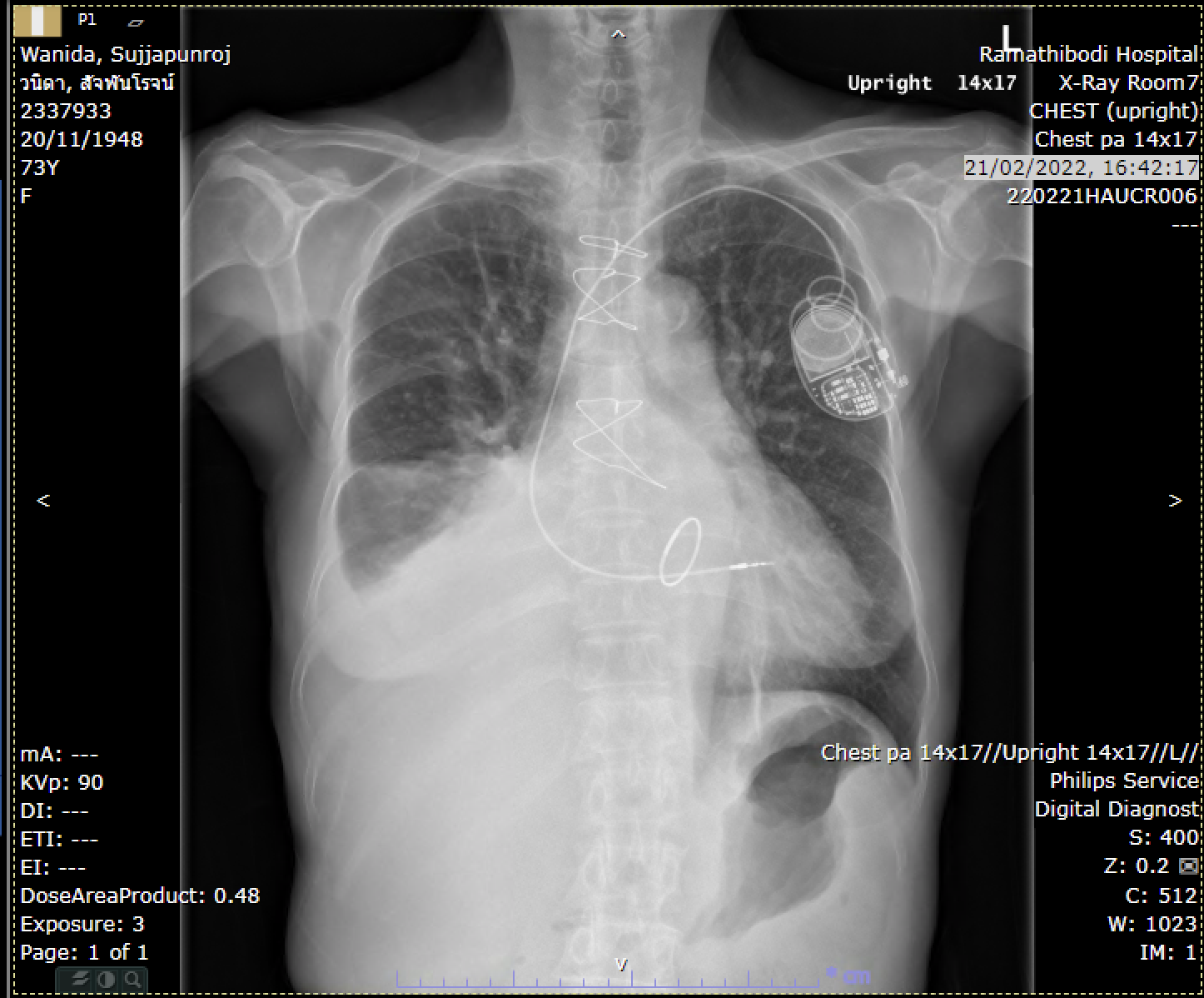
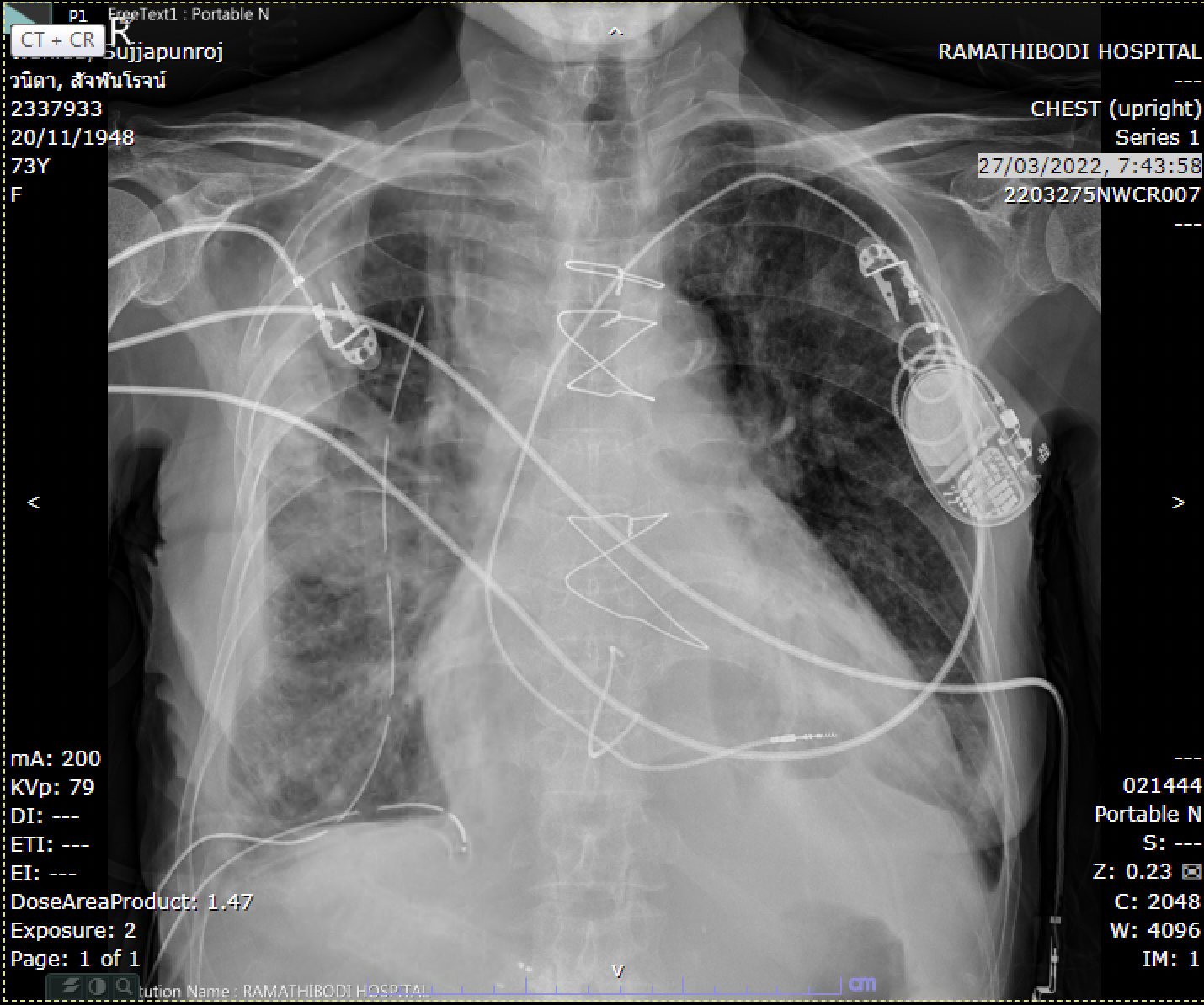
A 73-year-old woman, status post mitral valve repair and single chamber PPM placement 5 years ago, presented with dyspnea on exertion for 1 year. The TTE showed severe MR and severe TR, then she was admitted for elective mitral valve surgery (Mitral valve replacement with Epic size 25 mm)and tricuspid valve repair with Contour 3D annuloplasty band. During the postoperative period, she developed recurrent biventricular heart failure.
 SMA preop PLA12.mp4
SMA preop PLA12.mp4
Relevant Test Results Prior to Catheterization
The TTE revealed good biventricular systolic function, recurrent severe tricuspid regurgitation, and well-seated mitral valve prosthesis, however, there was faint abnormal color Doppler flow at the posterior aspect of the mitral valve. The CT scan showed a large pseudoaneurysm arising from the basal inferior wall(sub mitral valve ring) of LV, The diameter was 7.7 mm at neck and 25 x 49 x 41 mm in size.

SMA post op echo3.mp4
SMA post op echo10.mp4
Relevant Catheterization Findings
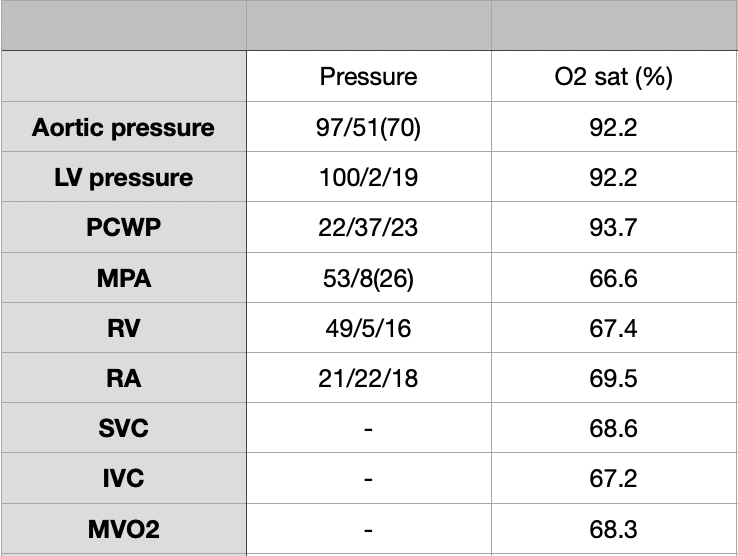
Combine left and right heart catheterization was done, showing elevated mean PCWP = 23 mmHg, LVEDP = 19 mmHg, mean RA pressure = 18 mmHg with giant V wave.The shunt run showed no significant step up, cardiac output 6 L/minute and cardiac index 4.6 L/min/m2. The left ventriculogram demonstrated a large sub-mitral LV pseudoaneurysm size 43 x 33 mm. The coronary angiogram showed no significant stenosis.
SMA dx.mp4
SMA dx2.mp4
Interventional Management
Procedural Step
Firstly, we scheduled to close the pseudoaneurysm with fluoroscopy and TEE guided. Heparinzation was done after vessel puncture to keep ACT > 250 seconds, and guiding JR4 with 0.035" Terumo wire was passed into the LV and then rotated clockwise to engage the neck of the pseudoaneurysm. After we could successfully pass the wire into the aneurysm, we inserted the guiding JR4 along the wire into the cavity. The Amplatzer vascular plug II was delivered via the guiding JR4 and deployed at the neck of the aneurysm. The final LV gram showed a significant reduction of contrast draining into the pseudoaneurysm. A week later, we brought the patient back to do the transcatheter tricuspid valve-in-ring using Sapien 3 size 26 mm. Right FV access was done with 14 F Edward Esheath, and the balloon wedge catheter was used to pass the tricuspid valve toward RV and PA to prevent cord entanglement. Amplatz superstiff was placed in the pulmonary artery for support and then the S3 was tracked along the stiff wire passing into RV. Because the Contour 3D ring was an incomplete ring with 3D curve, we concerned about the position and location of the S3 related to the ring after deployment. Therefore, LV pacing was done with Safari wire, the S3 was held and we rotate the tube to RAO and LAO to confirm the accurate position and its interaction during the balloon inflation. The following TTE and RV gram showed a well-seated of the S3 valve with mild paravalvular leakage.
SMA intra-op11.mp4
SMA Tviv 16.mp4
SMA Tviv 17.mp4
Case Summary
We reported the post-operative mitral valve and tricuspid valve surgery with submitral LV pseudoaneurysm and recurrent severe tricuspid regurgitation which were successfully treated by transcatheter Amplatzer vascular plug closure and transcatheter tricuspid valve-in-ring, respectively. The key step for submitral valve pseudoaneurysm closure is good pre-procedural planning and device selection. The JR or AL guiding catheters are suitable for engagement in the neck of the pseudoaneurysm. For valve-in-ring in this case, there was a challenge during the deployment due to the incomplete ring with the 3D curve of the ring. Multiple views during the deployment are useful in this situation.